 October
25
October
25
Tags
The Science of Stuttering
A special thank you to Kaja Bajc and Jaymie Horak for their incredibly helpful personal input.
How is it that someone can sing fluidly but struggle to introduce herself? Or smoothly imitate a foreign accent without trouble, but get stuck on words when speaking without pretense?
Stuttering is a communication disorder characterized by disruptions (“disfluencies”) in a person’s speech. These disfluencies can take on many different forms, such as repetition, prolongation, or stoppage of sound, sometimes accompanied by physical tension. It is a common misconception that stuttering arises from anxiety; the disorder is actually not primarily emotional or psychological in nature. Stuttering is instead primarily a motor disorder, a problem with the physical production of sound.

From [16]: “The left column shows speech waveforms (amplitude as a function of time); the right column shows a time–frequency plot using a wavelet decomposition of these data. In the top row, speech is fluent; in the bottom row, stuttering typical repetitions occur at the “B” in “Biology.” Four repetitions can be clearly identified (arrows) in the spectrogram (lower right)”
Studies of young children have shown that shyness does not predict development of a stutter [1], and children who stutter do not show higher levels of stress in social situations [2]. While some reports indicate higher levels of anxiety in adults who stutter [3], the anxiety is likely a product of the stuttering and not the other way around; a particular study found that heightened anxiety was limited to social situations involving speech [4], and therapy that reduced anxiety and improved psychological well-being in those who stutter did not reduce stutter severity [5].
Often stuttering first manifests in young children just learning to talk. In many cases, the stuttering is a transient phase; it is reported that while 5% of people will stutter at some time in their lives [6], the overall prevalence in the population at any given time is around 1% [7]. This means that usually stuttering does not persist into adulthood.
Why do people stutter?

The basal ganglia
There is no single cause of stuttering. While most incidences of stuttering arise during childhood, some adults who did not stutter as children can develop a stutter later in life due to a stroke, brain injury, or neurodegenerative disorder. While the correlation is by no means perfect, it seems that, in many cases, injury- or disease-related onset of stuttering involves injury or degeneration of a brain region called the basal ganglia [8-9]. Brain hypoxia (a lack of oxygen) can occur not only in adulthood but also prenatally, so it is possible that a portion of childhood stuttering is also due to brain injury.
The basal ganglia is a group of structures deep within the brain. It is known for its role in the planning and execution of movement and in orchestrating an appropriate balance between motor activation and inhibition. Two pathways help to strike this balance—the “direct” pathway activates movement, and the “indirect” pathway inhibits it. The neurotransmitter dopamine plays an important role in both pathways but has different effects based on which type of dopamine receptor it binds to. Injury, degeneration, or chemical imbalance in these basal ganglia pathways underlies many motor disorders such as Parkinson’s disease and Huntington’s disease.
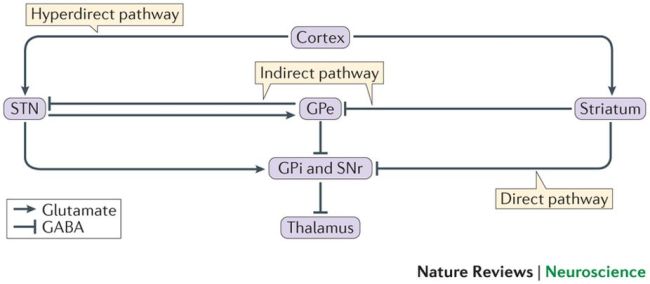
The structures of the basal ganglia interaction in “direct” and “indirect” pathways to coordinate movement. Abbreviations- STN: subthalamic nucleus; GPe: external globus pallidus; GPi: internal globus pallidus; SNr: substantia nigra pars reticulata. Image from [17].
Some hypothesize that those who stutter have an imbalance of dopamine signaling in the brain, throwing off the delicate coordination of motor activation and inhibition. This is likely only half of the story, though, as people who stutter do not generally have other motor deficits. A few pieces of evidence support the involvement of dopamine. For instance, a drug (haloperidol) that specifically blocks a particular type of dopamine receptor is the most commonly studied pharmacological treatment for stuttering and seems to improve speech fluency in some cases. Another drug (ecopipam) that acts blocks a different dopamine receptor has also shown promise in reducing stuttering.
Technically these drugs should have opposite effects on motor activity based on the different receptors they act on; this paradox suggests that a dopaminergic imbalance in either direction might contribute to stuttering. This idea is supported by a study on Parkinson’s disease patients which found that unusually low or unusually high levels of dopamine were associated with speech disfluency in patients. People with Parkinson’s were more likely to have stuttering-like speech disfluencies than healthy controls, and this was the case both before and after daily DOPA medication (DOPA is a dopamine precursor), corresponding to low and high dopamine levels, respectively [10]. This study helps to explain why some dopamine-related studies on stuttering have produced seemingly contradictory results.
There are still many gaps in our scientific understanding of stuttering, but a few clues lie in the fact that particular contexts seem to erase the stutter. While problems arise with spontaneous speech (speech to convey a message), people who stutter usually speak fluidly when speaking to the beat of a metronome, speaking in sync with a group, singing, imitating an accent, or talking to pets. These anomalies are explained by a prominent theory in stuttering research: the dual premotor systems hypothesis.
It takes two: the dual premotor systems theory
Decades ago, researcher Gary Goldberg proposed a distinction between two parallel neural pathways that precede movement, suggesting that these pathways are differentially activated depending on the context of the movement [11]. One pathway (the “medial” pathway) involves the basal ganglia and supplementary motor area. This medial pathway is called upon for goal-directed movement. The other pathway (the “lateral” pathway) involves the lateral prefrontal cortex and the cerebellum.

The Dual Premotor System
The two are thought to be functionally distinct in the context of speech: the medial pathway underlies spontaneous, internally motivated speech (speaking to express a thought) while the lateral pathway is activated for speech that is timed to an external stimulus (singing), that has increased voluntary control (imitating a foreign accent), or that has low semantic content (speaking when alone or to a pet or infant) [12]. It therefore seems that contexts that engage the lateral pathway rather than the medial pathway often present no problem to people who stutter—it is the medial pathway that generates difficulty speaking.
The dual premotor systems theory is corroborated by more recent imaging studies. A PET study showed that people who stutter have more activation in their cerebellum during speech than those who do not stutter [13]. Some have interpreted this to mean that, because their medial pathway is not performing well, those who stutter rely more heavily on the lateral pathway even during spontaneous speech. Interestingly, increased cerebellar activity is associated with more fluid speech in people who stutter [14], suggesting that engagement of the lateral pathway is a relatively successful compensation mechanism.
Another imaging study suggests a second method of compensation. While most brain functions occur on both the right and left sides of the brain (the notion of right-brained and left-brained people is a myth!), language is usually lateralized to the left side. Researchers have found that people who stutter show a lot of activation on both sides of the brain rather than mostly the left side [15]. This recruitment of other brain regions is likely another mechanism of compensation. However, it should be noted that it is often difficult for researchers to create a testing environment in which a person will stutter naturally, so imaging results must be taken with a grain of salt.
What are some treatment techniques?
Luckily, research and technology have brought us a long way from the 19th century, when stuttering “treatments” included an operation involving cutting out a piece of the tongue or fitting the patient with a tongue weight [12, 16]. Another brilliant strategy apparently involved slapping the unexpecting person in the face with the tongue of a slaughtered cow (?!) [12]. Unsurprisingly, these methods were quite ineffective.

From [16]: “On the left is a device by Gardner from 1899 to artificially add weight to the tongue (United States patent number 625,879). On the right is a more complex speech apparatus by Peate from 1912 (United States patent number 1,030,964).”
Before we delve into current treatment techniques, it is important to realize that stuttering is not necessarily something that requires “treatment.” The thoughts and ideas of those who stutter are no less powerful, and we as a society must recognize and acknowledge this.
However, for those who wish to reduce stuttering, there are many types of treatment techniques. As mentioned previously, some dopaminergic drugs have shown success in treating stuttering, but these are serious medications that often come with unwanted side-effects. Technology has provided interesting, safer options. Devices such as SpeechEasy (a hearing-aid type insert) alter the tone with which people hear their own voice and introduce a delay. This changes the auditory feedback in a way that leads the speaker to engage in a more chorus-like speech context, perhaps engaging the lateral pathway more than the medial pathway and thereby reducing stuttering. It does not work for everyone, but has been helpful for some.
Today, the most common treatment for adults who stutter is to work with speech language pathologists on techniques that help reduce the severity of the stutter. For instance, a common strategy is to practice prolonged speech in which the person tries slowly easing into a syllable that is presenting difficulty. Unfortunately, these learned techniques often lose their power over time; the stutter seems to evolve and adapt, finding its way back into speech. Many people therefore rely on other self-taught methods including word-swapping, changing breathing patterns, or just simply staying silent. While the former means that people who stutter often have a more extensive vocabulary than those who don’t, these methods can be exhausting at best and devastating at worst. No one should be silenced because of the way they speak.

Colin Firth as King George VI in The King’s Speech. The movie highlights King George VI’s struggle with stuttering and his close relationship with his speech therapist.
Therapy in the stuttering field is slowly shifting its focus to help those who stutter to accept their stutter, to recognize that it does not diminish the value of their words. To this end, the National Stuttering Association has support groups all over the U.S.; the motto of the organization is, “If you stutter, you are not alone.” Targeting the fear associated with speaking can often engender empowerment and improve mental health in a way that relentlessly fighting the stutter does not. Sometimes, accepting the stutter seems to eventually lead to a decreased frequency of stuttering.
As researchers uncover new information on successful natural compensation mechanisms for stuttering, new technology may provide better ways to train those who stutter to engage these compensation mechanisms better, more frequently, and more permanently than current techniques. In the meantime, we as a society need to learn to ignore how a person might sound and focus instead on what that person is saying.
References
-
Reilly S, Onslow M, Packman A, Wake M, Bavin EL, Prior M, Eadie P, Cini E, Bolzonello C, Ukoumunne OC. Predicting stuttering onset by the age of 3 years: a prospective, community cohort study. Pediatrics. 2009 Jan;123(1):270-7. doi:10.1542/peds.2007-3219.
-
B. van der Merwe, M.P. Robb, J.G. Lewis, T. Ormond. Anxiety measures and salivary cortisol responses in preschool children who stutter. Contemporary Issues in Communication Science and Disorders, 38 (2011), pp. 1-10
-
Craig A, Hancock K, Tran Y, Craig M. Anxiety levels in people who stutter: a randomized population study. J Speech Lang Hear Res. 2003 Oct;46(5):1197-206.
-
Menzies, R. G., Onslow, M., & Packman, A. (1999). Anxiety and Stuttering: Exploring a Complex Relationship. Am J Speech Lang Pathol, 8(1), 3-10. doi: 10.1044/1058-0360.0801.03.
-
Menzies RG, O’Brian S, Onslow M, Packman A, St Clare T, Block S. An experimental clinical trial of a cognitive-behavior therapy package for chronic stuttering. J Speech Lang Hear Res. 2008 Dec;51(6):1451-64. doi: 10.1044/1092-4388(2008/07-0070)
-
Andrews, G., & Harris, M. (1964). The syndrome of stuttering, Clinics in developmental medicine, No. 17. London: William Heineman Medical Books Ltd
-
Bloodstein, O. (1995). A handbook on stuttering. Chicago: Easter Seal Society.
-
Theys C, De Nil L, Thijs V, van Wieringen A, Sunaert S. A crucial role for the cortico-striato-cortical loop in the pathogenesis of stroke-related neurogenic stuttering. Hum Brain Mapp. 2013 Sep;34(9):2103-12. doi: 10.1002/hbm.22052
-
Ludlow CL, Rosenberg J, Salazar A, Grafman J, Smutok M. Site of penetrating brain lesions causing chronic acquired stuttering. Ann Neurol. 1987 Jul;22(1):60-6. PubMed PMID: 3631921.
-
Goberman AM, Blomgren M. Parkinsonian speech disfluencies: effects of L-dopa-related fluctuations. J Fluency Disord. 2003 Spring;28(1):55-70. PubMed PMID: 12706913.
-
Goldberg G. (1991) Microgenetic Theory and the Dual Premotor Systems Hypothesis: Implications for Rehabilitation of the Brain-Damaged Subject. In: Hanlon R.E. (eds) Cognitive Microgenesis. Springer Series in Neuropsychology. Springer, New York, NY
-
Alm, P. A. (2005). On the Causal Mechanisms of Stuttering Department of Clinical Neuroscience, Lund University
-
De Nil LF, Kroll RM, Houle S. Functional neuroimaging of cerebellar activation during single word reading and verb generation in stuttering and nonstuttering adults. Neurosci Lett. 2001 Apr 20;302(2-3):77-80. PubMed PMID: 11290391.
-
Sitek, K. R., Cai, S., Beal, D. S., Perkell, J. S., Guenther, F. H., & Ghosh, S. S. (2016). Decreased Cerebellar-Orbitofrontal Connectivity Correlates with Stuttering Severity: Whole-Brain Functional and Structural Connectivity Associations with Persistent Developmental Stuttering. Frontiers in Human Neuroscience, 10, 190. http://doi.org/10.3389/fnhum.2016.00190
-
Fox PT, Ingham RJ, Ingham JC, Hirsch TB, Downs JH, Martin C, Jerabek P, Glass T, Lancaster JL. A PET study of the neural systems of stuttering. Nature. 1996 Jul 11;382(6587):158-61. PubMed PMID: 8700204.
-
Büchel, C., & Sommer, M. (2004). What Causes Stuttering? PLoS Biology, 2(2), e46. http://doi.org/10.1371/journal.pbio.0020046
-
Jahanshahi M, Obeso I, Rothwell JC, Obeso JA. A fronto-striato-subthalamic-pallidal network for goal-directed and habitual inhibition. Nat Rev Neurosci. 2015 Dec;16(12):719-32. doi: 10.1038/nrn4038.
Basal ganglia image: https://www.neuroscientificallychallenged.com/blog/what-are-basal-ganglia
Dual Premotor Systems image: http://stutter-mind-body.blogspot.com/2011/04/stuttering-and-dual-premotor-system.html
The King’s Speech image: https://www.bbc.com/news/entertainment-arts-12093065

You must be logged in to post a comment.