 November
03
November
03
Get Over It: Discrimination and Mental Health
Prologue: This fall quarter at UC San Diego, the School of Medicine began its first elective course in mental health outreach for clinicians. I consider myself a rather fierce advocate for mental health care and illness awareness, so naturally I jumped at registering despite my already pretty full schedule. On October 11, 2016, I had the opportunity to conduct a presentation and workshop on the subject of discrimination and mental illness with fellow neurograd student Katie Fife in conjunction with two members of the UCSD faculty, Drs. Lisa Eyler and Rachel Robitz. The following recapitulates the information that we went over during the workshop, and if it resonates with you I strongly encourage you to check out the rest of this quarter’s events hosted by other students in the class! Details at the end of the post.
In a recent survey, it was estimated that approximately 43.8 million Americans have a diagnosable mental illness.[1] That’s nearly 1 in 5 American citizens, which means that even if you don’t have a diagnosis yourself, it’s overwhelmingly likely that somebody you know and care about has a mental illness of some kind. Despite these numbers, stigmatization and discrimination against people with mental health needs in this country is still alive and strong. Millions of Americans who go without mental health treatment each year, often because either the treatment is not accessible or they’re too intimidated by all of the vicious stereotypes to seek treatment at all. It can be incredibly difficult to understand what it’s like to face stigma and discrimination if you aren’t on the receiving end of it, but if you knew for (almost) certain that someone you love faces it every day, wouldn’t you want to?
 Despite the high rate of mental illness in our society, we are generally terrible at discussing it. At the private interpersonal level, we throw around mental health terms with little regard for what they actually refer to. I know I’m not the only one who’s heard people describe their one moody friend as “totally bipolar” or their organizational habits as “way too OCD.” It’s not that there’s necessarily any malice behind these statements; at this point “bipolar” and “OCD” are words that people throw around pretty readily. But if you actually have Bipolar Disorder or Obsessive-Compulsive Disorder, it’s probably pretty frustrating to have your chronic illness likened to the inconvenience of someone’s messy desk drawer. If you sprained your dominant hand and couldn’t use it for a couple of weeks, you wouldn’t say that you felt like an amputee to an actual amputee, would you?
Despite the high rate of mental illness in our society, we are generally terrible at discussing it. At the private interpersonal level, we throw around mental health terms with little regard for what they actually refer to. I know I’m not the only one who’s heard people describe their one moody friend as “totally bipolar” or their organizational habits as “way too OCD.” It’s not that there’s necessarily any malice behind these statements; at this point “bipolar” and “OCD” are words that people throw around pretty readily. But if you actually have Bipolar Disorder or Obsessive-Compulsive Disorder, it’s probably pretty frustrating to have your chronic illness likened to the inconvenience of someone’s messy desk drawer. If you sprained your dominant hand and couldn’t use it for a couple of weeks, you wouldn’t say that you felt like an amputee to an actual amputee, would you?
Public discourse on mental illness at the media level is almost worse. A highly disproportional amount of media coverage of mental illness is stories related to gun violence. As a result, more and more people have come to believe that mentally ill people are inherently more likely to be unpredictable and dangerous even though studies have shown that the vast majority of violent crimes are carried out by mentally healthy individuals.[2] Furthermore, mentally ill people are more likely to be victims rather than perpetrators of violent crimes, so if anything, they should be the ones we are working to protect rather than scapegoat. (The preeminent philosopher-satirist of our time, Mr. John Oliver, recently came out with a really good segment on media treatment of mental health issues on his show Last Week Tonight, and I strongly recommend taking ten minutes to give that a watch. Just remember it’s HBO before watching it with your kiddos.)

who else can you really trust for reliable news these days?
While stigma primarily encompasses negative attitudes and stereotypes, discrimination at the institutional level goes a step further. This kind of discrimination distinctly entails the restriction of rights and privileges of a certain group by a powerful few. Very generally speaking, this can be broken down into two categories: intentional, in which rules or policies of a private or public entity (like the government or an employer) consciously and purposefully restricts a group’s rights, and unintentional, in which the discriminating outcome seemingly results without the conscious prejudicial efforts of those in power.
It’s very likely you’ve heard the phrase “structural” or “institutional discrimination” relatively recently, as perhaps the largest human rights movement in our country at the moment (#blacklivesmatter) has been shining a bright light on the issue with regard to race. In fact, it can be very helpful to comprehend the consequences of structural discrimination against most any group through the powerful lens that #blacklivesmatter has created and focused for us. Consider for example a very clear and unfortunately recent example of blatant structural discrimination in our own nation’s history: Jim Crow laws. These are the laws that sustained segregation and restricted basic human rights like voting solely on the basis of race. Similarly restrictive laws exist for people with mental illnesses. As recently as the mid-90s, nearly 1/3 of American states had laws that restricted the rights of the mentally ill to hold elective office, participate in juries, and vote; and nearly ½ of the states had laws that limit the right of the mentally ill to marry or retain custody of their children.[3]
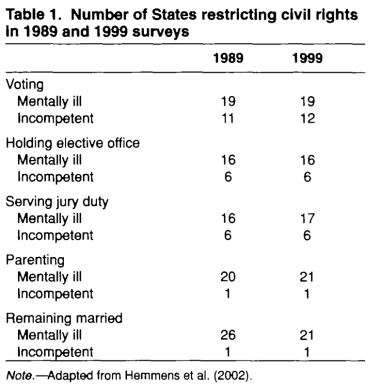
(Corrigan et al. 2004)
Here’s where the conversation starts to get tricky. One can argue that laws should exist that restrict the rights of mentally ill people. If someone suffers from major depression and the symptoms are so severe that they can’t reliably get out of bed and provide nutritious meals for their children, maybe they aren’t fit to be a parent at this time. If someone suffer from psychotic episodes that detach them from reality, maybe background checks should stop them from owning a gun. That said, many of you probably have one frustrated thought bubbling rapidly to the surface right about now: not all mental illnesses are created equal. Have you ever heard about how some cancers are pretty easy to treat but others can be extremely aggressive? It’s the same idea with mental illnesses. Not all cancers are the same, and not all mental illnesses are the same. A person suffering from delusions may not currently have the capacity to be an informed voter, yet someone with severe obsessive-compulsive disorder could have just as dense a psychiatric history as the delusional patient but be completely aware of the political issues and capable of voting responsibly. Furthermore, that same delusional patient probably won’t be detached from reality forever. A psychotic episode, while it can recur, is often transient. That person may have the capacity to be just as informed and responsible as anyone else, depending on the current state of their illness.
we can all use a friendly reminder to not compare apples and oranges from time to time.
To help prevent laws like these from painting with too wide a brush, it is helpful to draw distinctions between “mentally ill” and “mentally incompetent.” These terms differ in that the former is a medical diagnosis while the latter is a legal determination that is currently used to describe a person that is not capable of achieving certain community standards as a result of their illness. If the law states that a right or privilege does not pertain to the mentally ill, the law is preventing a group of sick individuals from exercising that right – not necessarily a group of people who have demonstrated that the right need be revoked. But then how do we classify mental incompetence? If we are to view mental illnesses as we do disabilities, then we can refer to the Americans with Disabilities Act (ADA): people with disabilities have the right to reasonable accommodation, and “one cannot be considered incompetent if these kinds of accommodations are not provided.”
Are we adequately accommodating mentally ill populations in this country? Unfortunately, we often are not, and this is where problems of unintended structural discrimination further complicate the picture. Perhaps the most consequential example of such discrimination against the mentally ill comes in the form of health care access and quality. Mental health research receives substantially less funding from the National Institutes of Health (NIH) than similarly prevalent medical conditions, like cancer. Many would argue that this fact alone automatically renders mental health care inferior to other forms of more heavily researched medical care. Furthermore, mental health care is historically more difficult to access in a cost effective manner. The Affordable Care Act (ACA, or Obamacare) made substantial improvements to previous attempts at mental health care improvement, such as the Mental Health Parity Act of 1997 which required mental health care coverage to be equal to that of medical or surgical health care – but only if the insurer was going to bother to provide mental health care at all. It wasn’t a requirement to have it, just to make sure it was just about as good as the rest of the plans if you did.
Obamacare made serious progress in the right direction by requiring mental health coverage in all insurance plans, allowing children to remain on their parent’s healthcare plan until age 26, including behavioral health in screening procedures, and preventing insurance denials based on pre-existing conditions. That said, there is still a lot of work to be done as mental health coverage continues to slip through the remaining cracks. Some insurance will pay primary care doctors more for a 10-minute appointment than it will pay a psychiatrist for an hour, and as such many mental health care providers no longer accept insurance. Furthermore, while you can’t be denied insurance for a pre-existing mental health condition, the insurance can still determine that particular services your doctor requests are “not medically necessary” and refuse to cover the treatment or procedure, and this happens disproportionately more often to mental health services.[4] Compound this with the fact that many psychiatric medications (such as antidepressants or antipsychotics) are considerably more likely to be placed on more expensive prescription tiers or not be covered at all, and you are left with a sick population whose health care needs are not being met. Is this reasonable accommodation? Or is it borderline negligence? How can you be considered incompetent if you can’t find the help you need no matter how hard you try?
There is a lot of information to process here, and there are a lot of gray areas with regard to contrasting mental illness and incompetence that raise questions we may not be able to easily answer scientifically or ethically just yet. If things are going to change, however, it has to start with changing the dialogue about mental health. We as a society have to learn how to talk about mental illness in a respectful and informed manner. History has shown us that even when public attitudes change, the law can be slow to follow, so there is really no benefit to delaying a shift in public perception. Some people that live with mental illness find themselves in situations where they have to keep their diagnosis quiet (for fear of losing their job, becoming a social outcast, and so on). Those of us who have experienced the challenges of mental illness firsthand or through a loved one and are in the fortunate position to be able to talk about it openly have the opportunity to take the reins on this advocacy. I don’t know how or when or how much our country’s view of mental illness will change during my lifetime, but no problem has ever improved with silence. Start a dialogue about what you know. Set out to learn about what you don’t. If you aren’t doing it to help yourself, I can virtually guarantee you’ll be helping someone important to you.
Mental Health Outreach for Clinicians hosts events every Tuesday evening at 5pm in the Medical Education and Telemedicine Building (MET) Room 215 on the UCSD School of Medicine Campus and will continue for the rest of the 2016 fall quarter. Topics vary each week but are always related to mental health care issues and problem solving. They also have free pizza ;).
References:
[1] National Alliance on Mental Illness. http://www.nami.org/Learn-More/Mental-Health-By-the-Numbers
[2] U.S. Department of Health & Human Services. https://www.mentalhealth.gov/basics/myths-facts/
[3] Corrigan, P.W., Markowitz, F.E., & Watson, A.C. (2004). Structural Levels of Mental Illness Stigma and Discrimination. Schizophrenia Bulletin 30(3):481-491.
[4] National Alliance on Mental Illness (2015). A Long Road Ahead: Achieving True Parity in Mental Health and Substance Use Care.

You must be logged in to post a comment.