 January
09
January
09
Reefer Madness?
The recent legalization of marijuana in Colorado and Washington makes this is a good time to think about the potential risks of marijuana consumption. Marijuana has a long and storied history of recreational use in humans (earliest evidence of its use is 4000 BC in China1). The popular image of marijuana today is as a benign recreational substance because of its extremely low rate of overdosing and mild withdrawal symptoms.
So why is marijuana a Schedule 1 drug, a drug that can earn you more than 80 years in prison? There are a variety of historical reasons for this prohibition, but one reason I will examine today is the centuries-old idea linking marijuana use to the onset of madness. At the time of the 1894 Indian Hemp and Drug Commission report the common practice was to attribute certain forms of madness to marijuana use and the popular notion was that marijuana caused insanity. A 1930’s movie called Reefer Madness illustrates the common belief that marijuana causes madness. The movie tells the story of high school kids preyed upon by unscrupulous drug dealers. The students descend into madness, engaging in a variety of horrible actions including rape, suicide, and manslaughter. But what does science have to contribute to this discussion on marijuana and madness?
Adolescent marijuana use and schizophrenia
Modern day concerns about madness & marijuana center on its connection with Schizophrenia/Psychosis. In this article I will mostly refer to schizophrenia but studies have various criteria for clinical symptoms, some of which are broader (like psychosis which is a more generic psychiatric term) or narrower (like schizophrenia which has more specific clinical requirements for diagnosis). In this article I will use the term schizophrenia for simplicity, but know that the exact symptoms included in each study can vary. There are two main types of symptoms associated with schizophrenia: Positive symptoms (symptoms which add to a person’s normal behavior) which include hallucinations and also negative symptoms (symptoms which subtract from a person’s normal behavior) which include withdrawal from social contact and feeling depressed. Estimates of the individuals with schizophrenia in the population range from 0.3-0.7%.
While there are reports that marijuana can cause acute schizophrenia-like symptoms, the cessation of marijuana in acute cases leads to a favorable rate of recovery. A more troubling idea is that marijuana use during adolescence alters brain development in negative ways. Adolescence is when marijuana use begins for many people (Figure 1). Around 40% of 9-12th graders report marijuana use at least once in their lives and marijuana use is currently greater than cigarette use in adolescents2. Schizophrenia, like most psychiatric illnesses, has an onset that is typically the combination of a genetic vulnerability to the condition coupled with the environment of childhood and adolescence.
First, the evidence that marijuana is a key environmental risk factor for schizophrenia in adolescents. Marijuana use is typically doubled in schizophrenics compared to the normal population3. This is hard to interpret because people with schizophrenia may just be more likely to seek marijuana, possibly because it helps alleviate their symptoms. But longitudinal studies that ask about marijuana use and then follow-up with the participants years later find that people who reported marijuana use in the earlier study are between 1.5-2.5 more likely to develop schizophrenia compared to non-users at the follow-up study4. If you only include people who used marijuana before the age of 15 the number increases to 3 times more likely5. If you only include heavy users, the number can jump to 6 times more likely6.
These longitudinal studies are suggestive but still not evidence of causation. However, in animal studies where tighter control of conditions can be achieved, a similar pattern of findings is observed. Animals exposed to cannabinoids during adolescence have increased symptoms which look like schizophrenia (like decreased pre-pulse inhibition) and mood disorders later in life7. Taken together, the human longitudinal studies and animal studies point to a relationship between early adolescent marijuana use and later development of schizophrenia in a subset of individuals.
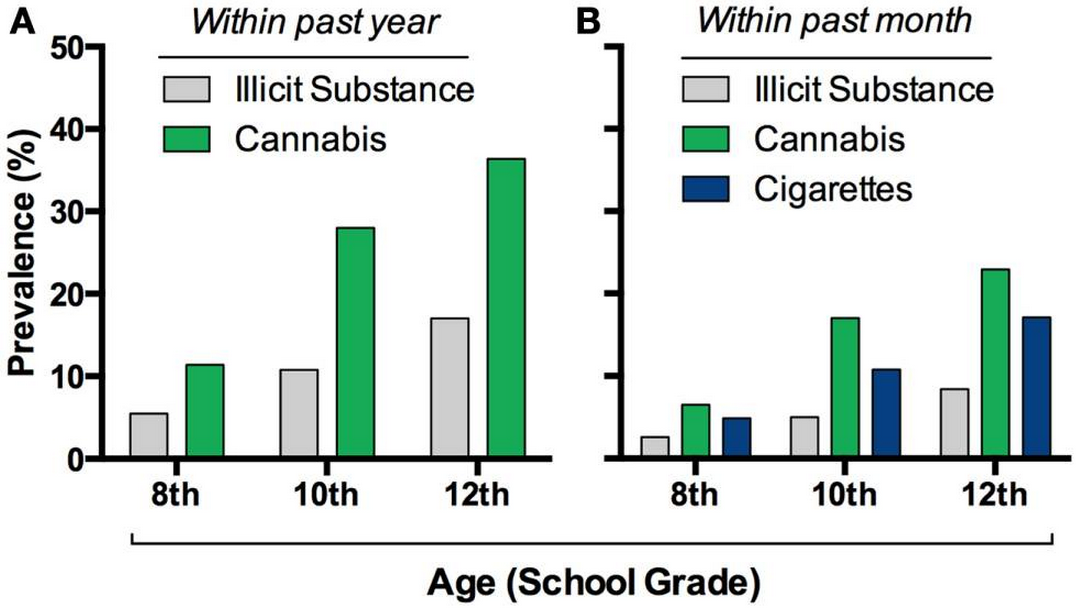
Figure 1. A) Adolescent use of marijuana is greater than other illicit substances B) Adolescents today are more likely to have used marijuana than cigarettes.
Pathways from Marijuana use to Schizophrenia
So where is marijuana having its effects in the brain? The system of neuroreceptors sensitive to marijuana in the brain is called the endocannabinoid system. Typically the cannabinoid receptors (CBR’s) act to limit the release of neurotransmitters8. The system’s distribution and actions implicate it in in a number of developmental processes. In embryonic and early childhood development it helps different parts of the brain link up through processes such as neuronal migration9. It also plays an extremely important role in adolescence (Figure 2) a period when the endocannabinoid system peaks and undergoes patterns of changes in important regions such as the frontal cortex, hippocampus, and striatum10. The amount of CBR gene expression in the brain decreases slowly from adolescence onward. All this suggests that a proper functioning endocannabinoid system is important for normal brain development during the window of adolescence.
The dysfucntion of GABA and dopamine is implicated in the development of schizophrenia. Normal endocannabinoid function works to inhibit GABA release in the frontal cortex. Marijuana may upset the balance of the endocannabinoid system leading to an change in the levels of GABA in the frontal cortex and impaired function in this region11. Elsewhere, dysfunction of endocannabinoid functioning on interneurons in other parts of the brain, particularly the mesolimbic regions, leads to increased release of dopamine12. As the individual becomes sensitized to excess dopamine coupled with frontal dysfunction, the system becomes increasingly unstable in that reward prediction is impaired and the brain has trouble in knowing where sensory signaling is coming from (i.e. hallucinations).
There is also a second theory regarding the developmental effects of cannabis on the brain which focuses on the thalamus. The thalamus can simplistically be thought of as a part of the brain which ‘connects’ many other parts of the brain by routing communication effectively between them. The thalamic theory broadly is that marijuana may compromise the ability of thalamic nuclei to effectively route information between different parts of the cortex. This is a key part of the condition of schizophrenia, as hallucinations consist of self-initiated activity being thought by sensory parts of the brain to be coming from outside sources. If the thalamus is not effectively communicating to sensory parts of the brain that activity is coming from the brain itself, this could be a key aspect of the delusions. The actual theory is much more detailed and complex, and I highly recommend reading the whole thing if you are interested (scientific review #3 in the references).
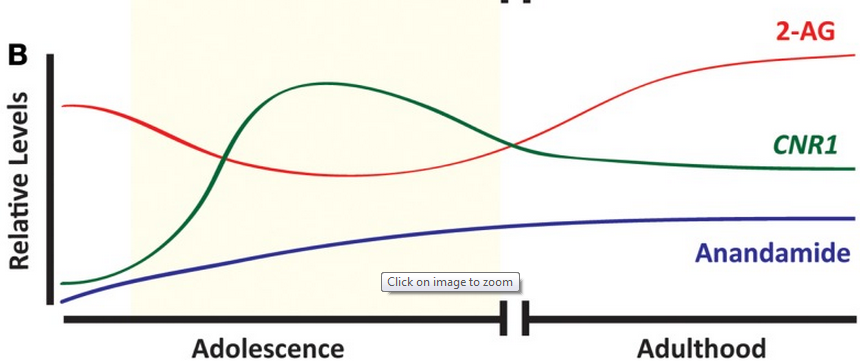
Figure 2. Three endogenous cannabinoid signals and their approximate levels across the lifetime. As seen during adolescence, the system is in flux and different than in adulthood. During this period correct functioning of the system is key to development of a well-functioning brain. It is here that marijuana use could have the largest effect on development of schizophrenia.
What does being it mean to be vulnerable to schizophrenia? There are two types of risk: genetic and environmental. Genetic risk has centered on the catechol-O-methyltransferase (COMT) gene13, although other genes such as AKT1 have also been implicated to lesser degrees. COMT codes for an enzyme that is involved in degrading neurotransmitters such as dopamine. How this gene interacts with marijuana is not well known, but having the valine variant in combination with adolescent marijuana use may make you more likely to develop schizophrenia. In terms of environmental factors, stress when young is implicated. This could include things like growing up in an urban environment or suffering childhood abuse14. Figuring out the exact interaction between marijuana and these other risk factors will be a difficult but necessary step to characterizing who is most at risk from adolescent marijuana use.
THC/Cannabidiol and Modern Marijuana
So far, we have been discussing marijuana as a monolithic construct. But there are at least 70 cannabinoids in marijuana. The one most people associate with marijuana is tetrahydrocannabinol (more commonly known as THC). But the second most studied cannabinoid which has been attracting more attention recently is cannabidiol.
Cannabidiol appears to confer some neuroprotective effects (in contrast to THC). One example is that the administration of cannabidiol in rats is associated with decreased drug-seeking behavior15. Further, cannabidiol has also shown protective effects against various symptoms of psychosis16. The distinction between these two different components of marijuana can be seen in the thalamic theory of schizophrenia. As the thalamus becomes more disordered, abnormal brain rhythms become more apparent in patients. Cannabidiol though may confer some of its neuroprotective effects by restoring normal rhythms. Modern marijuana plants are grown with increased THC and decreased cannabidiol and are thought to confer a higher psychosis risk, possibly increasing the risks posed by adolescent marijuana use.
Conclusion
Early cannabis use in adolescence has been associated with predisposing certain individuals to develop schizophrenia later in life. These individuals seem to have dysfunction in their frontal cortex due to GABA abnormalities, sensitization to dopamine in their mesolimbic structures, and dysfunction of thalamic relay of cortical information from one region to another. Genetic and environmental risk factors appear to play a key role in determining which individuals develop schizophrenia (a comparatively tiny percentage of all marijuana users) and which suffer no discernible problems. Further research is needed to decide exactly which individuals are vulnerable.
How does marijuana use affect the outcomes for patients who present with schizophrenia? There is a bidirectional relationship between marijuana and schizophrenia. This means that people with schizophrenia who try to quit marijuana use will be likely to relapse and use marijuana again while people who continue to use marijuana during treatment are more likely to have worse clinical outcomes17. If marijuana use stops at the first episode of schizophrenia-like symptoms recovery odds may be improved, but more evidence needs to be collected.
How to end this article? On the one hand, plenty of high-functioning people smoke marijuana and show no ill effects for it. But as with everything in life, actions do carry risk. This isn’t an anti-drug commercial full of gray images and ominous music where a disembodied voice drones ‘Bobby was going to lead a productive life, but then he smoked weed. Now he sits in the corner and hears voices. Marijuana: not even once’. But you should be aware that there is a growing scientific consensus that for some individuals marijuana carries risks beyond the playful Cheech and Chong image it has garnered in the popular media.
Sources
Scientific Reviews:
– Chadwick, B., Miller, M. L., & Hurd, Y. L. (2013). Cannabis use during adolescent development: susceptibility to psychiatric illness. Frontiers in psychiatry, 4.
– Burns, J. K. (2013). Pathways from cannabis to psychosis: a review of the evidence. Frontiers in psychiatry, 4.
– Vukadinovic, Z., Herman, M. S., & Rosenzweig, I. (2013). Cannabis, Psychosis and the Thalamus: Some New Theoretical Concepts and Insights. Neuroscience & Biobehavioral Reviews.
– Parakh, P., & Basu, D. (2013). Cannabis and psychosis: Have we found the missing links?. Asian Journal of Psychiatry.
Specific Papers:
1) Li, H. L. (1973). An archaeological and historical account of cannabis in China.Economic Botany, 28(4), 437-448.
2) Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2013). Monitoring the Future national results on drug use: 2012 Overview, Key Findings on Adolescent Drug Use. Ann Arbor: Institute for Social Research, The University of Michigan.
3) Hall, W., & Degenhardt, L. (2000). Cannabis Use and Psychosis: A Review of Clinical and Epidemiological Evidence∗. Australian and New Zealand Journal of Psychiatry, 34(1), 26-34.
4) Henquet, C., Murray, R., Linszen, D., & van Os, J. (2005). The environment and schizophrenia: the role of cannabis use. Schizophrenia bulletin, 31(3), 608-612.
5) Arseneault, L., Cannon, M., Witton, J., & Murray, R. M. (2004). Causal association between cannabis and psychosis: examination of the evidence. The British Journal of Psychiatry, 184(2), 110-117.
6) Van Os, J., Bak, M., Hanssen, M., Bijl, R. V., De Graaf, R., & Verdoux, H. (2002). Cannabis use and psychosis: a longitudinal population-based study.American journal of epidemiology, 156(4), 319-327.
7) Wegener, N., & Koch, M. (2009). Behavioural disturbances and altered Fos protein expression in adult rats after chronic pubertal cannabinoid treatment.Brain research, 1253, 81-91.
8) Freund, T. F., Katona, I., & Piomelli, D. (2003). Role of endogenous cannabinoids in synaptic signaling. Physiological reviews, 83(3), 1017-1066.
9) Harkany, T., Guzman, M., Galve-Roperh, I., Berghuis, P., Devi, L. A., & Mackie, K. (2007). The emerging functions of endocannabinoid signaling during CNS development. Trends in pharmacological sciences, 28(2), 83-92.
10) Mato, S., Del Olmo, E., & Pazos, A. (2003). Ontogenetic development of cannabinoid receptor expression and signal transduction functionality in the human brain. European Journal of Neuroscience, 17(9), 1747-1754.
11) Eggan, S. M., Mizoguchi, Y., Stoyak, S. R., & Lewis, D. A. (2010). Development of cannabinoid 1 receptor protein and messenger RNA in monkey dorsolateral prefrontal cortex. Cerebral Cortex, 20(5), 1164-1174.
12) Lupica, C. R., & Riegel, A. C. (2005). Endocannabinoid release from midbrain dopamine neurons: a potential substrate for cannabinoid receptor antagonist treatment of addiction. Neuropharmacology, 48(8), 1105-1116.
13) Caspi, A., Moffitt, T. E., Cannon, M., McClay, J., Murray, R., Harrington, H., … & Craig, I. W. (2005). Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biological psychiatry, 57(10), 1117-1127.
14) Kuepper, R. (2011). Do cannabis and urbanicity co-participate in causing psychosis? Evidence from a 10-year follow-up cohort study. Cambridge University Press.
15) Ren, Y., Whittard, J., Higuera-Matas, A., Morris, C. V., & Hurd, Y. L. (2009). Cannabidiol, a nonpsychotropic component of cannabis, inhibits cue-induced heroin seeking and normalizes discrete mesolimbic neuronal disturbances. The Journal of Neuroscience, 29(47), 14764-14769.
16) Leweke, F. M., Piomelli, D., Pahlisch, F., Muhl, D., Gerth, C. W., Hoyer, C., … & Koethe, D. (2012). Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia. Translational psychiatry, 2(3), e94.
17) Hides, L., Dawe, S., Kavanagh, D. J., & Young, R. M. (2006). Psychotic symptom and cannabis relapse in recent-onset psychosis Prospective study.The British Journal of Psychiatry, 189(2), 137-143.

Pingback: Cannabis, Creativity, & The Cortex | NeuWrite San Diego
To be complete your study should follow the rise of cannabis use in society vs the incidence of schizophrenia. i.e. where are the bodies? No bodies? No problem. Or at least minimal. Which is to say – not worth feeding the prison/industrial complex with bodies.
Your failure to deal with that issue seriously flaws your paper.
It reminds me of Donal Tashkin who was convinced (before he did the studies) that marijuana HAD to lead to cancer because the smoke had a number of known cancer causing agents in it. What he found was that smoking cannabis reduced the incidence of lung cancer.
And we are starting to see in the literature papers on treating schizophrenia with cannabis.
To be complete your study should follow the rise of cannabis use in society vs the incidence of schizophrenia. i.e. where are the bodies? No bodies? No problem. Or at least minimal. Which is to say – not worth feeding the prison/industrial complex with bodies.
Your failure to deal with that issue seriously flaws your paper.
It reminds me of Donal Tashkin who was convinced (before he did the studies) that marijuana HAD to lead to cancer because the smoke had a number of known cancer causing agents in it. What he found was that smoking cannabis reduced the incidence of lung cancer.
And we are starting to see in the literature papers on treating schizophrenia with cannabis.
Further: Your “Genetic and environmental risk factors appear to play a key role in determining which individuals develop schizophrenia (a comparatively tiny percentage of all marijuana users)” indicates that any study done must be quite large to get useful results. Consult with a statistician to insure that any study you do or cite is robust. Statistical mistakes by non-statisticians are extremely common. I read some where recently that something like 90% of medical studies done were useless due to unreliable statistics. That is quite a waste.
I believe it was a class in advanced statistics that did a survey and the estimates going in were that 30% to 50% of the studies would not have reached statistically valid conclusions. The actual results surprised all concerned. Of course they may not have looked at a large enough sample to reach a statistically valid conclusion. Which would be doubly ironic. Still. It is a cautionary tale.
I tend to agree that the use of CANNABIS by young people can have negative effects, especially on developing brains, but so can alcohol & too much TV ?
The thing I find fascinating in all the ‘studies’ is that none of them definitively agree that Cannabis causes mental illness (could be a contributing factor in people who overindulge). The whole premise of ‘Reefer Madness’ has been discredited as : Lies, Fallacies & Misinformation aimed at pushing an agenda that led to the current FAILED Drug War. Many of the studies in the 1960-70s were funded by companies to prove that Cannabis IS harmful, regardless of any possible positive attributes. Cannabis had been used medicinally for thousands of years. In 19th century New Zealand a Catholic Nun (Mother Mary Aubert) grew it & marketed a line of medicines that were widely used to treat a raft of illnesses, that are only now being REDISCOVERED.
Its time to end the Reefer Madness & move on, to the end of the WAR on DRUGS
Zedd,
A confounding factor in “cannabis is harmful to young brains” is that endocannabinoid production peaks in roughly the 15 to 25 year age cohort. Precisely the years when cannabis use peaks.
I have yet to find a good explanation for that correlation.