 March
11
March
11
Tags
Heavy on My Mind: Lead Poisoning (Part I)
A couple weeks ago, Chris Rock was faced with the formidable task of addressing the #OscarsSoWhite controversy at the Academy Awards. Typical of Rock’s stand up, his performance was met with mixed reviews. While he certainly did not shy away from the lack of diversity in Hollywood, his monologue had some missteps, including Stacey Dash, an unnecessary jab at Asians (who btw have received #OnlyOnePercent of Oscar nominations ever), and an assertion that the uproar against the awards show only occurred this year because in previous years, black people “had real things to protest! Too busy being raped and lynched to care about who won best cinematographer.”
The implication that Oscars snubs are the only protest-worthy acts of racism in the United States right now justifiably upset many viewers. And in fact, while Rock delivered his monologue, directors Ryan Coogler (of “Creed”) and Ava DuVernay (of “Selma”) with the Blackout for Human Rights collective held a benefit event, #JusticeForFlint, to raise awareness of the devastating water crisis in Flint, Michigan, a predominantly black city.
In case you missed it, in April 2014 (almost 2 years ago!), the city of Flint switched its water source from Lake Huron to the Flint River, ultimately leading to grotesquely high levels of lead (aka poison) in the city’s tap water (listen here for more). The situation is disgusting, but for a long time, I ignored it. I have no particular interest in the state of Michigan, and I just didn’t feel like being exposed to more upsetting news about our country, so, I willfully scrolled past the pictures of dirty tap water and the headlines about Flint’s sick and dying children for as long as I could.

I fear (read: know) that I am not the only person who has chosen to ignore the water crisis. It’s depressing and complicated. But it is also important, and not just about Flint. In this post, I will discuss the biological and economic costs of lead poisoning. Its effects are widespread throughout the body—and the United States—and I hope you will find them worthy of your attention.
Lead: What is it good for? Absolutely Nothing.iii
Essential elements are elements that are required for human life. There are 19 essential elements, including carbon, zinc, and sodium. Lead is not an essential element. We do not need it. It has no known biological function. But lead doesn’t just sit back and relax while the essentials do their thing. No! Lead actively works to prevent the good work of the essential elements, to our bodies’ detriment.
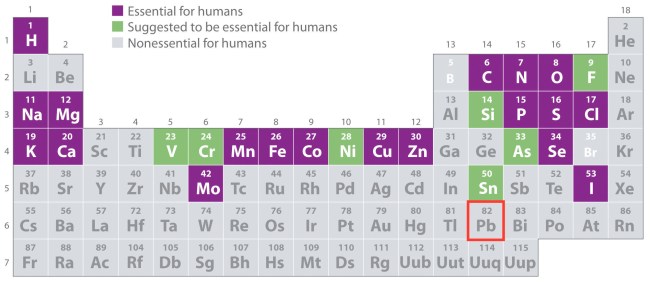
Lead = Pb. From UC Davis’s ChemWiki.
This is not news. We have known that lead is bad for over 2000 years. Seriously! Lead acetate is sweet, and one day, someone decided to add it to wine. This made people sick. And in the 2nd century BC, a Greek physician and poet named Nikander reported colic and paralysis resulting from heavily leaded wine (1,2). Despite this knowledge, lead acetate continued to be used as a sweetener. And a few hundred years (and many sick people) later, in the 1st century AD, Pliny the Elder also recorded the toxic effects of lead. Of course, Pliny’s warnings went unheeded, and the wealthy continued to enjoy their delicious and destructive wine. Wine so destructive that it has been implicated in the fall of Rome (3)! So, giving humans the benefit of the doubt, perhaps the people who knew about lead’s poisonous powers had all died and so could not prevent further incorporation of the evil element in our daily lives. In any case, the harmful effects of lead were eventually rediscovered—notably in 16th-century Germany, by Samuel Stockhausen and Eberhard Gockel (4). And yet, use of the toxin continues today! (For a poetic, if infuriating, story about the invention and devastating public health effects of leaded gasoline, I recommend Episode 77: Butterflies of the podcast the Memory Palace.)

The continued use of lead in anything just makes no sense at all.
Childhood lead poisoning was reported in the United States in 1914. By the 1940s, the long-term effects of acute lead poisoning were observed, and in the 1970s, the effects of subacute/subclinical levels of poisoning, such as behavioral and learning disorders, were reported. As the extent of lead toxicity was revealed, the use of leaded house paint and gasoline were banned in the United States (2). Even so, lead poisoning remains a huge public health problem and in 2010 was categorized by the Centers for Disease Control and Prevention (CDC) as a Nationally Notifiable Noninfectious Condition—along with cancer, carbon monoxide poisoning, pesticide-related illness and injury, and silicosis (lung disease caused by silica dust). Currently, approximately 600,000 children suffer from elevated blood lead levels (BLLs).
How much is too much?
What exactly are “elevated” BLLs? BLLs are typically measured in μg/dL—that’s microgram (1 millionth of a gram) per deciliter (1/10 of a liter). In the 1960s, the threshold for elevated, or toxic, BLLs for children was 60 μg/dL. We have since come to learn that much lower BLLs are also toxic. So, the definition of elevated BLL for children was decreased to 10 μg/dL in 1991 and again to 5 μg/dL in 2012.
But how much is that, exactly? Let’s consider a BLL of 5 μg/dL, for example, in a 150-lb woman.
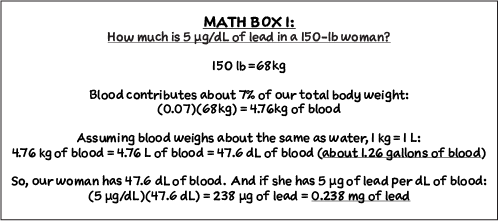
1 mg (aka 0.001 g) of lead is like a grain of sand. 0.238 mg is less than a quarter of a grain of sand. So picture ¼ of a “grain” of lead in a gallon of blood. That is more than 5 μg/dL. That is already more than too much.
Once it enters the bloodstream, lead has a half-life of 35-40 days (2,5). This means that 35-40 days after exposure, the amount of lead originally in the blood has decreased by ½. Therefore, BLL measurements only account for recent exposure. In the meantime, while some lead is excreted, more accumulates in bone. And the half-life of lead in bone tissue is about 20 years (6,7)!
Gross effects of lead poisoning
Lead can have many devastating effects in multiple organs, including the peripheral nervous system, heart, reproductive organs, liver, and kidneys. Poisoned adults may experience abdominal pain, loss of appetite, nausea, vomiting, arthritis, and hypertension (2,8,9). Weakness and paralysis can also occur in adults and children, leading to wrist or foot drops, which may be worse in patients concurrently suffering from sickle-cell disease (2,8). Children also have delayed onset of puberty (10–12), and as BLLs increase across a population, both height and hearing have been found to diminish (13,14).
During pregnancy and post-menopause, calcium and lead are “resorbed” (i.e., re-absorbed) from the bone into the bloodstream (7). Pregnant women—some of whom may have not had contact with lead for decades—may suffer stillbirths, neonatal death, birth defects, and decreased fertility rate (15). Men may have decreased sperm counts and teratospermia (aka abnormal sperm) (16).
Many changes occur in the brain, as well. Patients may exhibit increased clumsiness and staggering, clouded consciousness, headaches, and behavioral changes accompanying encephalopathy (aka general brain dysfunction) (2). Lead can cause edema (swelling) and herniation of the brain. This might occur due to increased vascular permeability and deterioration of the blood brain barrier (17,18). Lead can also alter myelin morphology, synaptogenesis, and neurotransmission through multiple pathways. Disruption to the cholinergic, dopaminergic, and glutamatergic neurotransmitter systems may lead to impaired learning and memory, which will be discussed in Part II.
Why is this happening?
Lead (Pb) usually exists in nature as a “divalent cation,” which means it has a charge of +2 and is called Pb2+ or Pb(II). Lead in this charged state binds strongly to sulfhydryl groups, which are sulfur-containing parts of proteins that are found throughout the body (e.g., in the amino acid cysteine). When lead binds to these proteins, as illustrated below, their structure and functions can be disrupted (2,8).
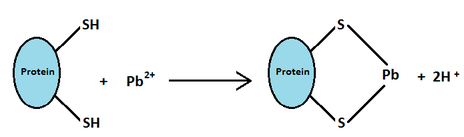
Lead interacting with sulfhydryl groups (-SH). From a Wikipedia article about ceramic glaze!
In addition to the overtly malicious manipulation of proteins, lead also works duplicitously as a stand-in for another divalent cation: calcium (Ca2+). Although it most often gets credit for keeping our bones strong (no small feat), calcium is also extremely important for many active processes throughout the body, and especially in the brain. Unfortunately, proteins that are meant to bind to calcium often preferentially bind to lead when it is available (19). But lead is not calcium! And many functions go awry due to lead’s ability to mimic or compete with calcium.
How do we protect our bodies from lead? Treatment options for lead poisoning are limited,v so our primary defense is to remove the element from the environment completely.
How much would that cost?
The decision to switch Flint’s water source from Lake Huron to the Flint River was made to save some money. But that plan horrendously backfired. Last week, Fitch Ratings reported that it will cost several billions of dollars to replace the lead pipes in the Flint region (and hopefully, eventually, the rest of the country).
That’s a lot of money, but several cost-benefit analyses of national lead poisoning prevention suggest that, now that the damage has been done, it will be well worth it to invest in preventative measures ASAP. For example, it has been calculated that every $1 invested in lead paint hazard control could have a positive return of $17 to $221, for a total savings of $181 billion to $269 billion (20). That is so much money!!
And yet, in 2012, drastic cuts were made to the Healthy Homes and Lead Poisoning Prevention Program.vi 😦
Below, I have reproduced some calculations by Landrigan et al. (21) for the estimated costs of pediatric lead poisoning in 1997. According to Landrigan et al., the environmentally attributable factor (EAF) for lead poisoning is 100%. This means that 100% of cases would be eliminated if environmental risk factors were reduced to the lowest feasible levels (22). For comparison, in the same study, the EAF was estimated at 30% for asthma, 10% for neurobehavioral disorders (including learning disabilities and developmental disorders), and just 5% for cancer.

According to this fairly conservative estimate (based only on loss of IQ and none of the other effects of poisoning), $43.4 billion was lost due to lead poisoning of 5-year-olds in 1997. And they were not the only ones being poisoned. Now, imagine the economic loss from lead-poisoned water in Flint. If we can mitigate that loss, the nation’s future economy will be much better for it.

Diagram by Salkever (23) illustrating the effects of lead poisoning on lifetime earnings, based on changes in IQ (used to for the calculations above).
What can we do?
Clearly, we have known for a long time that the lead situation in the United States needs to be handled. Although national average BLLs have been on the decline, BLLs in many communities continue to rise. This past Sunday, at the request of Hillary Clinton, the seventh democratic presidential debate was held in Flint to further raise awareness of the crisis. During the debate, Clinton announced that “We have a higher rate of tested lead in people in Cleveland than in Flint.” In fact, several cities have higher BLLs than Flint (I recommend this article to learn about some of those).
Unfortunately, the group that is most likely to suffer from high BLLs are preschool-aged black children of low-income families, living in old urban housing (8). In 1975, in a study on the “Relationship of Diet to Lead Poisoning in Children,” Mooty et al. (24) asked, “Why are the children of the poor [economically deprived Blacks and Puerto Ricans] being poisoned while their middle-class predecessors [in the same neighborhoods] were not?” Over 40 years later, Ava DuVernay answered that ongoing question when she stated that the situation in Flint is “environmental racism… We wouldn’t have seen this problem if this was in a community with more voice.” The poisoned children and their families have very little political power. They cannot afford a renovated house, bottled water, and a protective dietv. And they cannot afford to fight lead poisoning alone.
These are facts. As someone privileged enough to spend my non-working hours writing a blog post (like you, who are privileged enough to read it 🙂 ), I hope I have used some of my resources to spread awareness about the lead crisis in America. I encourage you to explore some of the links above, watch the 4.5 hour #JusticeForFlint benefit, contribute financially if you can, and help give a voice to the voiceless!
And don’t forget to come back in a few weeks for Part II, in which another NeuWriter will discuss the learning, memory, and behavioral consequences of lead during development.
(P.S. Scroll down or click here for footnotes and Bonus Content that I couldn’t fit into the article!)
While Our #JusticeForFlint Event is Over, the Fight for Water & Democracy in Flint Continues https://t.co/Y5fwNgQdbq pic.twitter.com/bzDgvxKTN2
— #JusticeForFlint (@UnitedBlackout) March 6, 2016
References:
If you’d like access to any of the articles referenced in this post, please don’t hesitate to contact me!
- Meyer PA, Brown MJ, Falk H. Global approach to reducing lead exposure and poisoning. Mutat Res. 2008;659(1-2):166–75.
- Needleman H. Lead poisoning. Annu Rev Med. 2004;55(1):209–22.
- Gilfillan SC. Lead poisoning and the fall of Rome. J Occup Med. 1965 Feb;7(7):53–60.
- Eisinger J. Lead and wine. Eberhard Gockel and the colica Pictonum. Med Hist. 1982;26(3):279–302.
- CDC. Summary of Notifiable Noninfectious Conditions and Disease Outbreaks — United States. MMWR Morb Mortal Wkly Rep. 2015;62(54).
- Barry PS. A comparison of concentrations of lead in human tissues. Br J Ind Med. 1975;32(2):119–39.
- Silbergeld EK, Schwartz J, Mahaffey K. Lead and osteoporosis: Mobilization of lead from bone in postmenopausal women. Environ Res. 1988;47(1):79–94.
- Markowitz M. Lead poisoning: a disease for the next millennium. Curr Probl Pediatr. 2000 Mar;30(3):62–70.
- Menon AV, Chang J, Kim J. Mechanisms of Divalent Metal Toxicity in Affective Disorders. Toxicology. Elsevier Ireland Ltd; 2015;339:58–72.
- Williams PL, Sergeyev O, Lee MM, Korrick SA, Burns JS, Humblet O, et al. Blood lead levels and delayed onset of puberty in a longitudinal study of Russian boys. Pediatrics. 2010 May;125(5):e1088–96.
- Gollenberg AL, Hediger ML, Lee PA, Himes JH, Buck Louis GM. Association between lead and cadmium and reproductive hormones in peripubertal U.S. Girls. Environ Health Perspect. 2010;118(12):1782–7.
- Selevan SG, Rice DC, Hogan K a, Euling SY, Pfahles-Hutchens A, Bethel J. Blood lead concentration and delayed puberty in girls. N Engl J Med. 2003;348(16):1527–36.
- Schwartz J, Angle C, Pitcher H. Relationship between childhood blood lead levels and stature. Pediatrics. 1986;77(3):281–8.
- Schwartz J, Otto D. Blood lead, hearing thresholds, and neurobehavioral development in children and youth. Arch Environ Health. 1987;42(3):153–60.
- Bellinger DC. Teratogen update: Lead and pregnancy. Birth Defects Res Part A – Clin Mol Teratol. 2005;73(6):409–20.
- Vigeh M, Smith DR, Hsu PC. How does lead induce male infertility? Iran J Reprod Med. 2011;9(1):1–8.
- Struzyńska L, Walski M, Gadamski R, Dabrowska-Bouta B, Rafałowska U. Lead-induced abnormalities in blood-brain barrier permeability in experimental chronic toxicity. Mol Chem Neuropathol. 1997;31(3):207–24.
- Wang Q, Luo W, Zheng W, Liu Y, Xu H, Zheng G, et al. Iron supplement prevents lead-induced disruption of the blood-brain barrier during rat development. Toxicol Appl Pharmacol. 2007;219(1):33–41.
- Simons T, B. Cellular Interactions Between Lead and Calcium. Br Med Bull. 1986;42(4):431–4.
- Gould E. Childhood lead poisoning: Conservative estimates of the social and economic benefits of lead hazard control. Environ Health Perspect. 2009;117(7):1162–7.
- Landrigan PJ, Schechter CB, Lipton JM, Fahs MC, Schwartz J. Environmental pollutants and disease in American children: Estimates of morbidity, mortality, and costs for lead poisoning, asthma, cancer, and developmental disabilities. Environ Health Perspect. 2002;110(7):721–8.
- Smith KR, Corvalán CF, Kjellström T. How much global ill health is attributable to environmental factors? Epidemiology. 1999;10(5):573–84.
- Salkever DS. Updated estimates of earnings benefits from reduced exposure of children to environmental lead. Environmental research. 1995. p. 1–6.
- Mooty J, Ferrand CF, Harris P. Relationship of diet to lead poisoning in children. Pediatrics. 1975;55(5):636–9.
—–
Bonus Content:
i. Lead is not the only problem with the drinking water in Flint. Other problems include the presence of E. coli, which led to three boil-water advisories, extreme chlorine treatment, and consequently high levels of carcinogenic total trihalomethanes—all very much in violation of the Safe Drinking Water Act. (Note: the chlorine treatment contributed to the corrosion of the lead pipes, leading to elevated lead levels in the drinking water. This should have been expected, since it already happened in Washington, D.C., but Flint officials chose not to add corrosion-control chemicals to the water.)
ii. Shoutout to the residents of Flint, in particular LeeAnne Walters, whose “extreme citizen science” helped to bring the situation in Flint to light.
iii. To be fair, lead is actually useful sometimes. For example, in lead-acid batteries and lead shielding from radiation. But thankfully, lead-free alternatives for these products are on the rise!
iv. How likely are we to inhale dust particles? Or eat them? In 2008, Levin et al. reported that lead paint and dust accounted for 70% of elevated BBLs in children in the United States (25). The remaining 30% of lead can come from a variety of other sources, including gasoline and corroded water pipes. Additional sources of lead include but are not limited to:
- solder (used for plumbing, automobiles, toys, and food cans)
- ceramics (including wine jugs)
- Plastics
- nonallopathic (i.e., “alternative”) medicines
- Cosmetics
- Batteries
- Ammunition
- fishing weights
If any of these products are chewed, licked, or teethed upon, the consumer risks poison. Most readers might not have a problem keeping non-nutritive objects out of their mouths, but if you have ever been near a teething child or someone with pica, you will understand that it’s not so easy for everyone. Furthermore, the above listed products also give off dust, which can be breathed, and their residues can seep into surrounding soil, which can also be eaten or inhaled.
A list of recalled products from the U.S. Consumer Product Safety Commission can be found here. If you search through the “Primary Violations,” you can see all of the Children’s toys recalled due to the presence of lead. It is sickening. But at least they’re trying?
v. For BLLs greater than about 40 mg/dL, chelation therapy may be an effective means to increase lead excretion from the body (2,8). Lead binds to chelating agents, such as EDTA and succimer, so it cannot act on the body and is excreted in urine. But chelating agents can also increase lead absorption from the environment, so this treatment must be provided in a completely lead-free environment, which may be impossible for many patients. Chelation therapy is not permanent and is not effective for lower BLLs, so it is not commonly used.
Dietary intervention is a much more accessible means of treating elevated BLLs. In particular, low-iron and low-calcium diets result in increased lead absorption. Therefore, iron- and calcium-rich foods will help combat lead absorption (18,26). Unfortunately, the composition of our favorite calcium source, milk, may increase lead absorption (27). Thankfully, milk is not the only source of calcium! The Hurley Medical Center in Flint published the “Nutrition & Lead: Recipe and Resource Guide” for anyone who might need some help selecting and preparing lead-fighting foods.
vi. The budget for the Healthy Homes and Lead Poisoning Prevention Program has increased since 2012 but is still short of the $29 million budget before 2012. The National Safe and Healthy Housing Coalition is requesting a $35 million budget for 2017.
Bonus References:
- Levin R, Brown MJ, Kashtock ME, Jacobs DE, Whelan EA, Rodman J, et al. Lead exposures in U.S. children, 2008: Implications for prevention. Environ Health Perspect. 2008;116(10):1285–93.
- Goyer RA. Nutrition and metal toxicity. Am J Clin Nutr. 1995 Mar;61(3 Suppl):646S – 650S.
- Stephens R, Waldron HA. The influence of milk and related dietary constituents on lead metabolism. Food Cosmet Toxicol. 1975 Oct;13(5):555–63.

Pingback: Heavy on my Mind: Lead Poisoning (Part II) | NeuWrite San Diego