 October
24
October
24
Tags
Is Addiction a Disease?
While it may not seem obvious, this question carries a great deal of emotional weight to sufferers of addiction, as well as their families and friends. The answer to one question – Is addiction a disease? – seems to hold the answer to yet another question: Are many of the hurtful things I’ve done as a result of being addicted ultimately my fault? Did my shameful actions arise from an illness within my thoughts and brain, or my own incompetence and moral failure?
When Does it Matter?
Historically, addiction has been treated as a result of a flawed personality, or weakness of character – but modern psychology is looking at it more like a medical problem, or a candidate illness to be treated with professional help[1] . This question of how to approach addiction and people who suffer from it is important for a significant number of people, though important differently for people in different roles. For medical and psychological professionals, for example, what addiction is informs what treatment options are encouraged and offered. For researchers and insurance companies, it informs funding of existing or prospective treatment approaches. For family, friends, and users struggling under addictions’ hold, it informs perspective for our interactions with the people we care about, or the constant obstacles a recovering addict’s mind must combat daily.
“If you don’t know where you are going, you’ll end up someplace else.”
-Yogi Berra
If we want to know if addiction is a disease, it makes sense to first define what a disease even is. Unfortunately, the technical answer does not seem too clear – definitions are typically too precise to include a lot of things that intuitively are obviously diseases, while others are so wide-ranging they seem to include anything that ever happens to a person. My personal favorite definition doesn’t actually come from medical professionals, but from Merriam-Webster:
Disease (noun): a condition of the living animal or plant body or of one of its parts that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.
While a good place to start, potentially this definition is too vague for many readers’ taste. I think it is for me. Nonetheless, I do think it illustrates an important point by appearing perhaps intentionally broad – to ensure inclusion of most (or all) things typically considered diseases, as well as another important group of ailments: mental disorders.
“Well… Just, stop?”
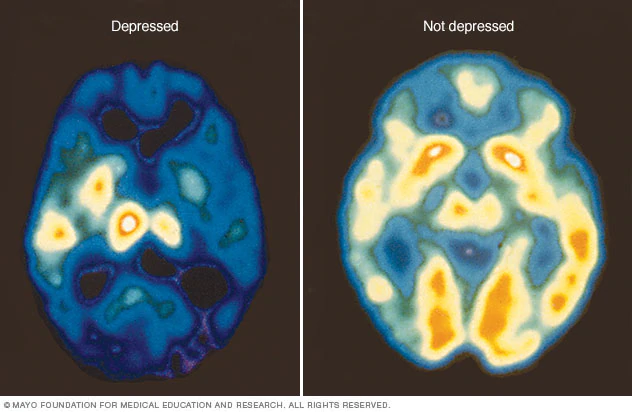
Comparative brain scans of a patient with depression and one without. Color indicates relative activity level of a given region, here we see dramatic decreases in the depressed patient across most of the brain.[3]
One of the first pieces of advice a person suffering from mental illness is likely to receive is actually not a very good piece of advice: “Just stop.” Obsessive Compulsive Disorder is not fun for people afflicted. Socially anxious people know it is a problem and seek solutions and strategies. Depressed people tend to, like most people, not want to be depressed – even if they have become so accustomed to depression that at times they may forget what life is like without it. So it makes sense that cures for these mental maladies are not as simple as making a decision to stop being debilitatingly compulsive, anxious, sad, or whatever it may be. Clearly the sufferer has already tried that. Instead, there are thousands of people spending their entire professional lives trying to figure out the best way to overcome various mental illnesses, or when a cure is not possible, manage symptoms in the hopes of making life with illness less uncomfortable.
There are, for people with health insurance in the western world, significant resources available to address mental health issues like depression, anxiety, and OCD. Your general practitioner, psychologists, psychiatrists, hell, even your local fitness and yoga instructors have numerous tools developed with the specific goal of helping improve mental health. Still, with the considerable pharmaceutical options, talk-therapy practices, brain scan differences, and just general, medical advice available to aid dealing with mental illness, largely, these ailments are not classified as “diseases”. They are mostly referred to by psychiatrists as disorders: Major Depressive Disorder (MDD), Obsessive Compulsive Disorder (OCD), Generalized Anxiety Disorder (GAD), Bipolar, Dissociative, Borderline Personality Disorders… the list goes on. This designation as disorder vs. disease is at times arbitrary, like based on who first identified and described the condition and when or where they did so. In the case of psychiatry, many illnesses that affect the brain and behavior do not have clear, demonstrable causes, or causes that are true for every and all patients – so the term disorder is used intentionally instead of disease, to serve as “a constant reminder that our knowledge of the nature of psychiatric illnesses is rather superficial.[4]”
Importantly, at least to me, this is not a judgement of what it is like to battle addiction, other mental disorders, or physical illnesses that are or aren’t technically “diseases.” And once afflicted, I do not see a difference in the empathy nor vigilance a cancer patient or addict deserve to show themselves, or deserve to expect from medical professionals. It seems that western medicine takes a similar stance.
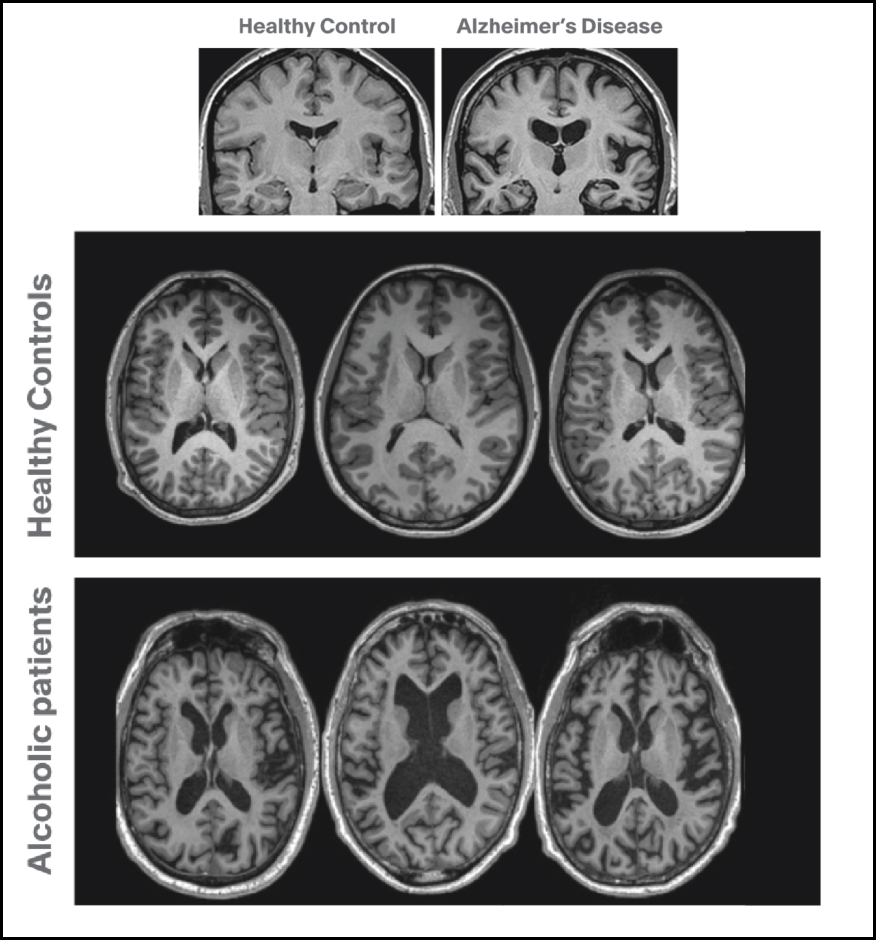
Top: Brain scans of a healthy patient next to an Alzheimer’s Disease patient. Black areas are areas without cells – which are dramatically larger in AD due to cell atrophy and death. Bottom: Scans of healthy brains compared to brains from patients with Alcohol Use Disorder. The dark areas show a similar increase in size – again due to cell atrophy and some death. Fortunately, abstinence from alcohol can allow these patients’ to recover much of that lost area as cells heal and regain their size and strength over time.[5]
The American Psychiatric Association (APA) publishes a collection of diagnostic criteria to guide psychiatrists in recognizing and treating mental disorders; their guidebook is now in its fifth edition and known as the DSM-5. The DSM-5 lists a category of disorders collectively called Substance Abuse Disorders, with 11 potential diagnostic criteria (listed below). Unsurprisingly this list includes some side effects common to physical addiction: frequent use, increased tolerance, or withdrawals when stopping use. These signs of bodily dependence on the drug differ from further important behavioral symptoms, which include cravings when sober, engaging in hazardous behaviors in pursuit of drugs or while on them, relationship problems arising from their use, or missing out on normal activities to use instead.
DSM-5: Symptoms of Substance Abuse Disord[6]
1) Hazardous use: You’ve used the substance in ways that are dangerous to yourself and/or others, i.e., overdosed, driven while under the influence, or blacked out.
2) Social or interpersonal problems related to use: Your substance use has caused relationship problems or conflicts with others.
3) Neglected major roles to use: You’ve failed to meet your responsibilities at work, school, or home because of your substance use.
4) Withdrawal: When you’ve stopped using the substance, you’ve experienced withdrawal symptoms.
5) Tolerance: You’ve built up a tolerance to the substance so that you have to use more to get the same effect.
6) Used larger amounts/longer: You’ve started to use larger amounts or use the substance for longer amounts of time.
7) Repeated attempts to control use or quit: You’ve tried to cut back or quit entirely, but haven’t been successful.
8) Much time spent using: You spend a lot of your time using the substance.
9) Physical or psychological problems related to use: Your substance use has led to physical health problems like liver damage or lung cancer, or psychological issues, such as depression or anxiety.
10) Activities given up to use: You’ve skipped activities or stopped doing activities you once enjoyed in order to use the substance.
11) Craving: You’ve experienced cravings for the substance.
No single person necessarily experiences all of these symptoms – the DSM actually divides into mild, moderate, or severe Disorder based on the number of symptoms a person is experiencing (2, 4, or >6, respectively), no matter which specific symptoms nor the order in which they appeared. Furthermore, the specific diagnosis a person receives depends on the drug of choice, e.g. Alcohol use disorder, stimulant use disorder, opioid, cannabis, tobacco, and so on. The specific category of Substance Use is important, as while all persons afflicted show similar risk signs and some shared strategies for recovery, the specifics of their path to moderation or abstinence reliably vary based on the drug (or behavior) of choice.
The variability in what to expect from one addiction to another is reflected in the brain too: different behaviors/drugs cause different changes in circuitry and neuronal health. The specifics of each addiction are still being investigated, in both animals (who, like us, will readily become addicted to drugs when isolated or stressed [7]) and humans. And while the specifics may differ, the pathways in the brain that underlie feelings of accomplishment, satisfaction, comfort, joy – collectively, the “reward circuitry” – are consistently altered during prolonged addiction. That is to say, things that would not be extremely gratifying to the average person suddenly become of the utmost importance to an addicted brain (see top-left image below), while normally important relationships and activities lose their draw in the process. These shocking, at-times appalling decisions commonly associated with ongoing addiction are therefore not just shared choices and behaviors, but shared choices and behaviors with corresponding changes in brain circuitry that arise during the addiction’s development.
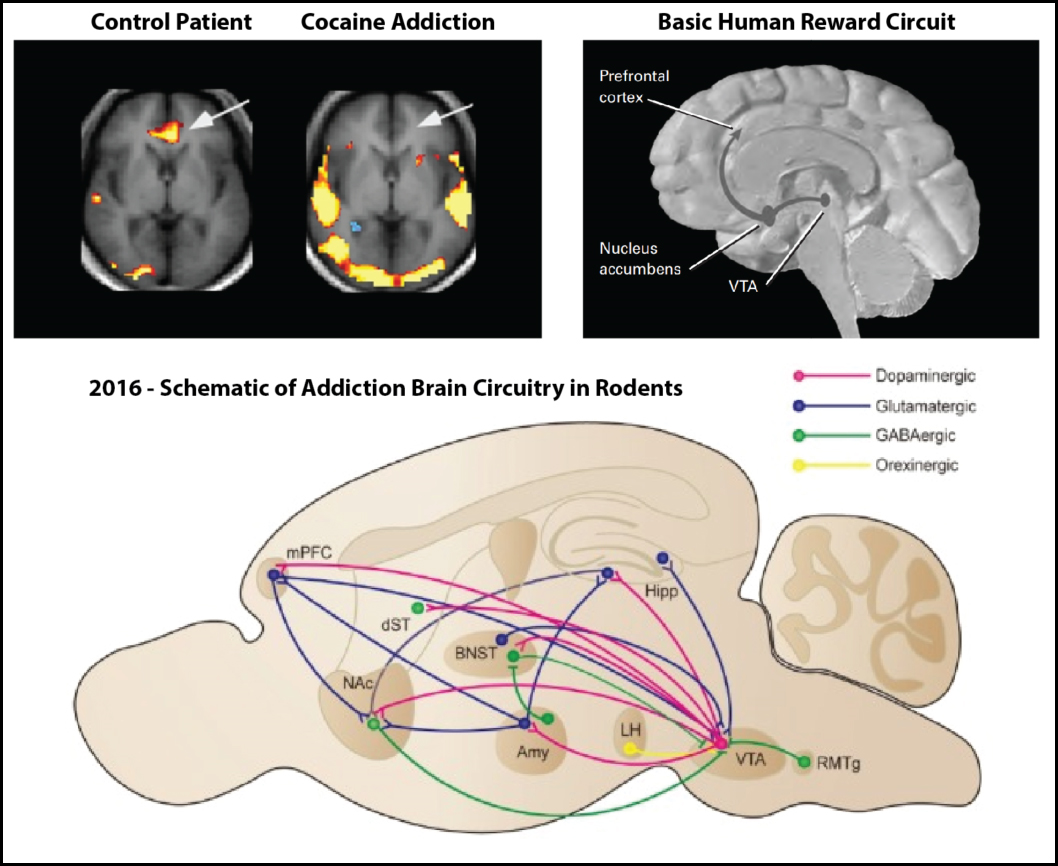
(Top left[8]) Areas of the brain that show increased activity when the patient just sees cues in a movie related to cocaine use. Arrows point to the prefrontal cortex. (Top Right[9]) The three main players in the “mesolimbic dopaminergic” reward circuit of the human brain. (Bottom[10]) An overview of addiction pathways as discovered and described in rodent models of addiction. Includes of medial Prefrontal Cortex (mPFC), Nucleus accumbens (NAc), and VTA – but through studying animals, we see significant cross talk throughout many more brain regions. There’s a lot here for different drugs to change differently!
And what does this all sound like? Earlier we called a disease a condition of the living animal or plant body or of one of its parts that impairs normal functioning and is typically manifested by distinguishing signs and symptoms. Again, this definition then does not seem constrained to just bacteria or viruses, but to include significant changes in behavior or activity, whatever the cause. To include many socially-accepted mental health problems. To include the brain chemistry of an addicted laboratory animal. And to include, it seems, Substance Use Disorders.
So… Is Addiction a Disease then?
Clearly addiction fits the bill by Merriam-Webster’s definition – is that good enough? For me personally, after all this… I am not convinced that addiction is a disease, though I really can’t put my finger on exactly why. Partially it may be because I feel lost in the semantics – at this point I’m not even sure what a disease is, and I cannot find a “perfect” definition that fits my intuition. Honestly, after thinking, researching, and writing about the topic, now I’m not even sure that cancer is a disease (can we literally unwittingly grow our own disease out of ourselves?), and unsure when a genetic disorder becomes a disease (do you have the disease from birth because of your genome? Even if you never show symptoms?). I’m not even sure that choosing to use drugs disqualifies substance use from becoming a disease when use turns into addiction – if someone forgets to wash their hands around a sick coworker, or has unprotected sex with a partner carrying a disease, does their choice to engage in risky behavior make the flu or HIV not diseases? Why or why not?
What are the criteria?
With a professional life steeped in biology research, what I have read and experienced in the realms of mental health and addiction, and the physical health scares every person, child, and grandchild personally witnesses, still I cannot confidently say outright that addiction is or is not a disease. In fact, it seems like I have actually reasoned myself out of being able to describe why even things that are obviously diseases are diseases, or why certain other ailments are not.
The reality is, however, that after months or years of substance abuse, users’ brains are demonstrably functioning in an altered state. Some behavioral differences persist well beyond drug withdrawal – users can spend months, years, or decades relying on a substance, and have to learn entirely new approaches to the difficulties and mundanities of daily life without. It can be an uphill battle. But the brain can and does rewire. Which does lead us to some good news: with consistent lifestyle change, things can and do get better. The bad news is I still can’t tell you if you’re getting better from a disease or not.
The last bit of news is that, ultimately, I don’t think the technical answer to this question really matters.
__________
Further Reading: If you are or think you might be battling addiction and are looking for further resources, the first recommendation is to visit your doctor. They will know the local resources, groups, etc. available for you, local therapists if need be, and can discuss medication if that is a route you and they wish to go. Advice online is only so useful – a medical professional can tailor to you specifically.
12-Step programs in your area are very easy to find searching online and full of welcoming people. Additionally, SmartRecovery.org is a non-religious, non-12-step organization that includes online meeting options, for people in the throes of addictive drug use or behaviors as well as their families and friends looking for help, and will help direct you to local meetings in your area (for local San Diego readers – smartrecoverysd.org).
And lastly, thank you for taking the time to read this article; I hope it may make you, your loved ones, or the world at large make a little more sense, even if I couldn’t find us a definition of disease.
Works Cited
[1] National Institute on Alcohol Abuse and Alcoholism. Alcohol Use Disorder. https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/alcohol-use-disorders
[2] Merriam-webster.com/dictionary/addiction
[3] Mayo Clinic. PET scan of the brain for depression. https://www.mayoclinic.org/tests-procedures/pet-scan/multimedia/-pet-scan-of-the-brain-for-depression/img-20007400
[4] John Cooper. Disorders are different from diseases. World Psychiatry. Feb 2004. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1414656/
[5] Lundbeck Institute. David Nutt, Imperial College London. Brain Imaging for Psychiatrists, Part 2: Structural (static) measures. https://institute.progress.im/en/content/brain-imaging-psychiatrists-part-2-structural-static-measures
[6] American Psychiatric Association. Diagnostic and Statistic Manual of Mental Disorders (DSM-5). https://www.psychiatry.org/psychiatrists/practice/dsm
[7] Bruce K. Alexander. Rat Park Versus the New York Times. https://www.brucekalexander.com/articles-speeches/rat-park/282-rat-park-versus-the-new-york-times-2
[8] Kim, J. et al. Brain Reward Circuits in Morphine Addiction. Mol Cells 2016. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5050528/
[9] Bettinardi-Angres, K. & Angres, D. Understanding the Disease of Addiction. National Council of State Boards of Nursing. https://www.ncsbn.org/Understanding_the_Disease_of_Addiction.pdf
[10] Wexler, BE. et al. Functional Magnetic Resonance Imaging of Cocaine Craving. Am J Psychiatry 2001. https://www.ncbi.nlm.nih.gov/pubmed/11136638

Pingback: Fighting fire with fire: How we can use opioids to fight opioid addiction | NeuWrite San Diego