 July
22
July
22
Tags
Shaken memory
image source: http://epilepsycongress.blogspot.com/2018/07/epilepsy-and-memory-loss.html
Like any college student in his early 20’s, I had a bit of a wild streak with alcohol back in April of this year (2021), getting drunk off my a**. That lasted about half a week. As I have written in a previous article, I suffer from a condition known as posttraumatic epilepsy (PTE), and the morning after one of my late nights out, I had another seizure (which probably traumatized my roommates). Here is how that day went, as relayed to me by my roommates, because I remember nothing that happened after the seizure.
I got up early that (fateful) morning, and rushed out of my room to go to the bathroom across the hall. I stood in the bathroom for a bit, and that is the last memory I have from that morning. At the same time, my roommate was in the kitchen making breakfast. After I had run into the bathroom, they heard multiple bangs in the walls, so they decided to check what was happening. They walked over to the bathroom, knocked on the door and asked if I was ok, and after no response from me, decided to open the door. To their shock, they found me lying there, convulsing on the floor. After calling 911, both of my roommates now tried to get me out of the bathroom (we had a tiny bathroom, so I had fallen in a way such that I was lying with my neck crooked against the wall). They later told me that the total seizure lasted about 10 minutes. After I stopped convulsing, I became aware, but was very confused. Once the EMTs were in the apartment , they helped me walk to the common area of the apartment, and sat me down on one of the chairs. Here is the brief conversation that followed (told to me by my roomates):
EMT [to me]: Donovan, do you know where you are?
Me: San Diego
EMT: Do you know what year it is?
Me[confused]: No…why don’t I remember what year it is?
Upon hearing my roommates tell me about what happened, I was aghast. How could I not remember entire conversations hours after having them? As someone who studies neuroscience, this intrigued me: I knew what the basic neuroanatomical structures and neurophysiology of memory and amnesia were, but I had not studied anything about a brief lapse of memory following a seizure. So I did a bit of research into epilepsy, memory, and amnesia. Before I get into the specifics of my case and what I found from this research into it, I feel it may be best to give a brief rundown of these basic neuroanatomical structures responsible for memory. Then, what will follow will relay what I found relating to what I experienced, to see if it gets me any closer to the answers to my questions.
Memory in the Brain
Memory is a very complicated phenomenon in the brain, with many different structures responsible for many different aspects and types of memory; thus, memory research in neuroscience is extensive and many questions are still being asked and researched. While we will touch upon some notable types of memory and their associated structures, for the purposes of our discussion right now, we will be focusing on the structures in the brain involved in memory consolidation and storage.
Explicit vs Implicit memory
When we think of memory, we think of things like remembering facts about the world around us (like how the sea cucumber ejects its internal respiratory organs at a predator when threatened), or stuff that we have learned from school (like having to memorize all of the countries in central and south america for spanish class), or events that we remember vividly (like the time you went on vacation to Las Vegas with your significant other). These are examples of explicit memories, which can be subdivided into declarative (facts) and episodic (events) memories, and this includes remembering facts about your past (autobiographical memory). However, implicit memories–those memories that you do not have conscious access to but still retain the information–also are an important part of our lives. Implicit memories mostly take the form of remembering how to do a task or action you’ve learned, such as riding a bike, which are known as procedural memories. As I could do things like walk and talk normally, I think it is safe to say that I didn’t have any impairment of my implicit memory (although the EMTs didn’t ask me to ride a bike, so who knows).
Neurological structures that contribute to the formation and storage of memory
The structures in our brain that are responsible for the key processes of memory are mostly within an encompassing structure known as the hippocampal formation. While there is still debate on which substructures actually make up this region, I will take it to include structures such as the hippocampus (proper), dentate gyrus (DG), subiculum (SUB), which are all important important for processes such as memory formation, memory storage, as well as working memory. The hippocampus itself is also divided into 4 regions (CA1-CA4), which all have been shown to play different roles in the recollection of recent and remote memories. DG contributes to the formation of new memories–similar to the hippocampus–and SUB has been found to influence things like working memory and spatial relations and/or memory. In addition, recent research into the organization of memories within the hippocampal formation has shown another function of SUB.
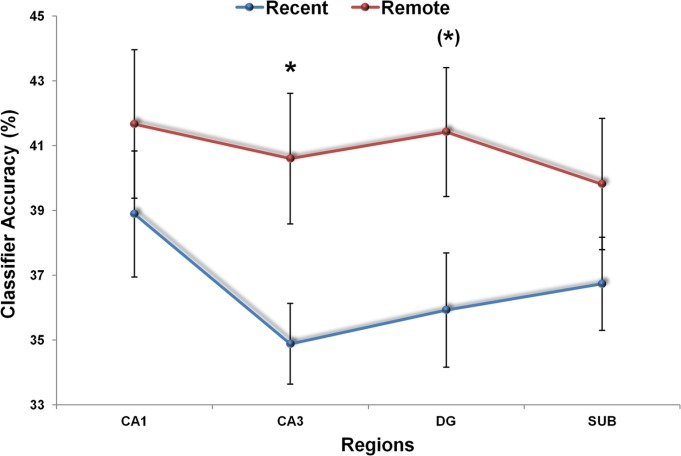
Researchers have found similarities and differences in the recall of memories within these regions. Whereas neuroimaging results show that both recent and remote memories were represented similarly within regions CA1 and SUB (Figure 1a), regions CA3 and DG show more response to information recall from only remote memories (Figure 1b) (Bonnici et al., 2013). With these findings, we can see that overall, CA1 and SUB represent recent memories more, while CA3 and DG represent remote memories more. Moreover, a curious finding about SUB that could be connected to my case is that SUB also plays a role in some cases of epilepsy. Now we have to ask, what research has been done into epilepsy’s effects on memory?
Epilepsy and Amnesia
DISCLAIMER: None of the conjectures I make about my case in this section are meant to be taken as official diagnoses: these are just simple observations and connections I draw from knowledge of the functions of the structures I have described and recent research into memory and epilepsy.
Now that there is a basic understanding of the types of memory, how they work, and what structures in the brain subserve each type, I will now come back to researching what may have been the cause of my condition. Let me begin with eliminating some of the more common forms of amnesia that could possibly relate to my situation: first, transient global amnesia (TGA). TGA is a condition that only affects memory for a brief amount of time, but completely affects short term memory (memory that can last only seconds) and possibly older memories as well. So, an individual with TGA could “recall only the last few moments of consciousness”. Although, as the name implies, this is a condition that only affects an individual for a short period of time (generally 2 to 8 hours), this condition also is characterized by repetitive questioning due to “dense” anterograde amnesia (which is the loss of ability to create new memories) (Butler & Zeman, 2009) . My roommates did not mention me repetitively questioning anything, so I think it less likely that TGA was involved in my case here. Following from that, the characterization that an individual “recalls only the last few moments of consciousness” does not seem accurate for my situation, considering I was able to carry out a conversation with the EMTs and not get confused.
Through further research, I also found a condition known as transient epileptic amnesia (TEA). This condition is characterized by “recurrent, brief (usually < 1 hour) amnesic episodes” (Butler & Zeman, 2009); being that a) this has been the only time this has occurred to me, b) this episode lasted more than 1 hour, and c) I have not experienced any other signs of this condition (olfactory hallucinations, automatisms, persistent memory deficits), this does not seem to be a reasonable diagnosis in my case. As well, this condition is not described as being preceded by a generalized seizure (convulsions).
Since these conditions do not seem to answer my question, looking at how the different stages of a seizure have been described may be another place to investigate. An article published in the Journal Epilepsia sets out to describe an operational definition for what is known as the postictal state, the period of time after the ictal period of a seizure, which in a generalized seizure is characterized by convulsions. The authors of this article state that it has been difficult to specify what precisely characterizes the postictal state due to “the challenges of identifying exact onset and termination points” (Pottkamper et al., 2020). While we are not concerned with the exact onset and termination points of the postictal state in this article, an article by Pottkamper et al. (2020) does give us a comprehensive overview of what characterizes the postictal state of a seizure. Specifically, the researchers list “declined alertness and short-term memory” as a clinical manifestation of the postictal state, under “cognitive dysfunction”. Closer to our answer? Possibly, but not quite.
While I do not believe this was a case of TEA or TGA, I do believe this seizure could have originated in the temporal lobe of my brain, since much of this lobe is responsible for our capacity for memory (the medial temporal lobe in specific, which includes all of the structures I described earlier) and recognition of various things (faces, certain objects, places, etc.). One curious detail that leads me to believe this lies within my answers to the two questions the EMTs asked me: the fact that I was able to remember what city I was in but not what year it was indicates that I was suffering from some form of temporally graded retrograde amnesia (TGRA), or loss of memory only up to a year prior to the current moment. More precisely, TGRA “refers to a phenomenon of…memory loss whereby information acquired (Clark et al., 2002). But why do I not remember this episode, answering any of the questions or going to the hospital? Well, let’s think about it: I have lived in San Diego my whole life, so it makes sense that this fact may be stored deep in long term memory (possibly CA3 or DG). However, what year it currently is is a more recent memory, as this incident occurred only four months into the year, meaning that this information may have still been stored somewhere in CA1 or SUB, as research has shown recent memories more likely to be accessed in these regions than others within the hippocampal formation. Since hippocampal damage is thought to cause difficulty remembering events that have recently occurred (anterograde amnesia), the fact that I do not remember any of the events that happened after my seizure that morning also lends itself to the temporal lobe being affected, if we remember that the hippocampus and DG are located within the temporal lobe. Therefore, some impairment of the medial temporal lobe must have lingered, most probably in either CA1 or DG, even though I was cognitively functional otherwise.
The brain and its capacity to store and process memories is extraordinary. Just as well, the findings and realizations that arise when the brain is not functioning properly are just as fascinating. Epilepsy has played a major role in the study of memory in neuroscience, so much so that the first finding that the hippocampus is linked to the formation of memories was discovered because the hippocampus, and therefore short-term memory, was removed from a patient with severe epilepsy to help curb the seizures originating in that area of his brain (patient HM). While I do not know if what I experienced that day was what I have described in this article, more research into epilepsy and memory can surely help get closer to answers for these peculiar cases.
References
Bonnici, H. M., Chadwick, M. J., & Maguire, E. A. (2013, June 27). Representations of recent and remote autobiographical memories in hippocampal subfields. Wiley Online Library. https://onlinelibrary.wiley.com/doi/full/10.1002/hipo.22155.
Butler, C., & Zeman, A. (2009). Syndromes of Transient Amnesia. The Neurology of Consciousness, 6(4), 339–351. https://doi.org/10.1016/b978-0-12-374168-4.00025-3
Clark, R. E., Broadbent, N. J., Zola, S. M., & Squire, L. R. (2002, June 1). Anterograde Amnesia and Temporally Graded Retrograde Amnesia for a Nonspatial Memory Task after Lesions of Hippocampus and Subiculum. Journal of Neuroscience. https://www.jneurosci.org/content/22/11/4663.
Pottkämper, J., Hofmeijer, J., van Waarde, J. A., & van Putten, M. (2020). The postictal state – What do we know?. Epilepsia, 61(6), 1045–1061. https://doi.org/10.1111/epi.16519
Squire, L. R. (2009, January 15). The legacy of patient H.M. for neuroscience. National Center for Biotechnology Information Search database. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2649674/.
Wikimedia Foundation. Wikipedia.

Interesting, thanks for sharing