 May
04
May
04
Tags
Shape of you – neuroscience of body image perception
The rise of Ozempic
“Everybody looks so great. When I look around this room, I can’t help but wonder: Is Ozempic right for me?” Jimmy Kimmel joked during his Oscars monologue earlier this year.
Ozempic, or Wegovy, or Mounjaro, has become quite popular in the last year. A drug primarily used for treating type 2 diabetes, it is also being used for its “convenient” side-effect of weight loss. Semaglutide, which is the active ingredient of Ozempic, promotes insulin release and regulates blood sugar levels (hence its use for diabetics), and also inhibits appetite and slows down emptying of the stomach (hence its role in inducing weight loss and treating obesity). A weight loss drug for obese individuals seems like a godsend, particularly one which not only reduces weight but also encourages a healthy lifestyle. What could possibly go wrong? Cue the Hollywood A-listers, social media influencers and everyone else obsessed with weight loss, which hiked up the demand to such an extent that the drug became unavailable or inaccessible to the people it was meant for. Not only is the supply chain broken, but now the drug is overpriced, and is no longer covered by health insurance due to its utilization for the purposes of vanity.
Weight loss and weight loss drugs are not necessarily the bad guys here, particularly in cases of extreme obesity where the individual’s health is suffering. Sometimes diet and exercise alone are not enough to reduce weight, and ‘external’ methods such as bariatric surgery (digestive system surgeries to help with weight loss) and weight loss drugs can help the delicate process of weight loss and management. When obese and overweight individuals are prescribed Ozempic by their doctors, they report dramatic improvement in their overall quality of life and health. They move better, breathe better, eat better and sleep better. It really is a wonder drug which improves their lives beyond recognition.
The problem here is that we as a society have normalized taking medication to look a certain way. Medication whose side-effects include nausea, constipation and brain fog. Medication that one has to inject into the bloodstream every week, because who knows what will happen to the weight if you stop? Medication whose long-term effects we know nothing about. Jimmy Kimmel’s joke is a perfect summation of how obsessed we are with losing weight, and of how being slim is considered good-looking.
This begs the question – why are we so obsessed with the way we look, particularly in terms of body weight and shape? Thousands of Instagram and Tiktok posts focus not only on losing weight, but also on achieving a body shape that is the trend of the season – be it slim, slim-thick (slim at the waist with a full hip) or BBL body types. These days with increased social media usage and scrutiny, people are insecure not only about their weight, but also about the sizes and shapes of specific body parts – lips, breasts, eyebrows, hips, thighs, nose, muscles – the list is endless [1]. People go to drastic lengths to conform to these ever-fluctuating ‘ideal’ body shapes. There are cultural and historical reasons for ‘slim’ being the preferred ideal body shape across the world. However, at the heart of these socio-cultural issues lies the concept of body image. Here I explore the neuroscience and psychology of body image, and how distortions in these processes can cause people to resort to drastic measures of weight loss – which often come with serious consequences, from using medication for vanity, to suffering from body dysmorphia and eating disorders.
Body dysmorphic and eating disorders
Body dysmorphic disorder (BDD) is a psychiatric illness characterized by intense preoccupation with imagined defects in appearance, which are not necessarily noticeable to others. While this can be related to any part of the body, a majority of cases involve obsessing over facial features, constantly monitoring and trying to ‘fix’ these issues, which can develop into distressing obsessive and compulsive behaviors. Eating disorders (ED) are characterized by dysfunctional eating behavior, stemming from body image issues and dissatisfaction pertaining to body size, weight and shape. The most common and well-known among these is anorexia nervosa (AN, check out this Neuwrite article to learn more about anorexia), which also has an additional symptom of denial and refusal of weight gain measures despite severe emancipation. Both BDD and ED arise due to body dissatisfaction and have similar symptomatology and psychiatric elements [2].
Who am I: The body and the self
Let us take a closer look at how body image is represented in the mind. Cognitive psychologists describe as many as six body representations that together form a coherent picture of the body in the mind [3]. We are all born with the innate, inflexible and non-conscious representation of the body, termed ‘body schema’, which is experienced as an awareness of the body to be a separate and independent entity from surrounding space. More nuanced representations develop over the course of life, as we perceive the body in relation to the world around us. ‘Objectified body’ which integrates our own and others’ perceptions of the body’s physical appearance, is a body representation arising due to social interactions. Body image is a representation thought to arise by comparing the objectified body with an ideal body (social comparison) dictated by socio-cultural norms.
Components of body image
Body image itself is thought to have two components: perceptual body image, which represents how accurately an individual can estimate their physical dimensions, and attitudinal body image, which represents how they feel about their body [4]. Cognitive psychologists are engrossed in a debate whether these two components are independent of each other. After all, it is possible that AN patients overestimate their size because they feel terrible about it, or they feel terrible about their size and hence overestimate it.
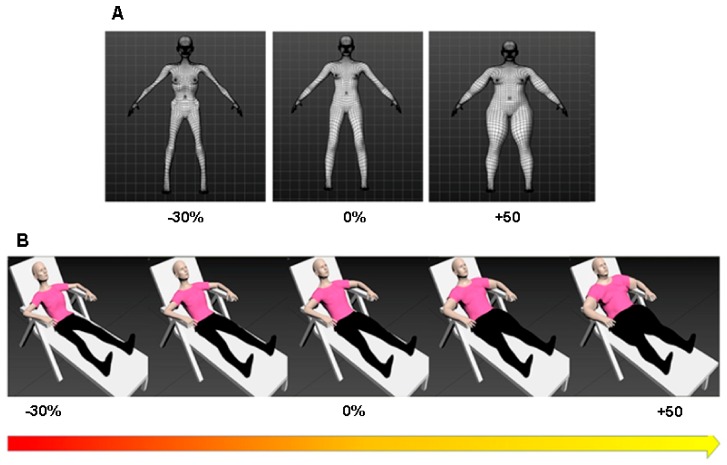
Irrespective of which side of the debate they are, psychologists have performed some clever experiments to understand what might cause AN. In one study, a group of AN patients and healthy controls were asked to match their body size to their own virtual reality-generated avatars of different sizes (-30% body weight to +50% body weight, Figure 1). Both groups estimated their sizes accurately. However, the AN group self-reported to be more dissatisfied with their own body size [5]. This shows that AN occurs due to the attitudinal change in body image rather than incorrect body size estimation.
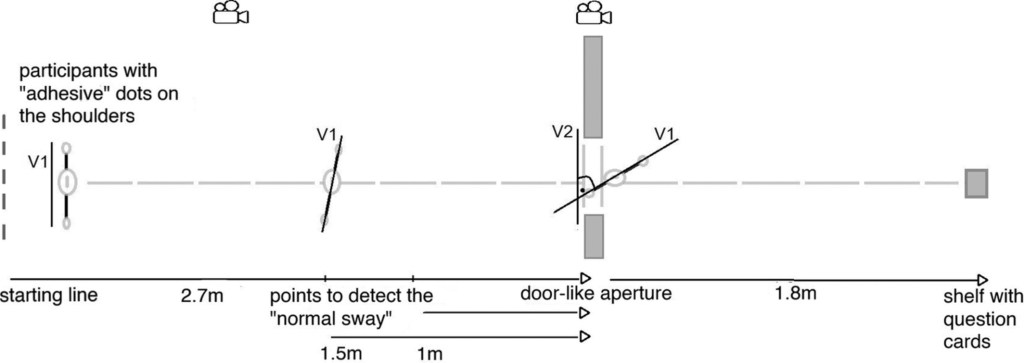
However, another study aimed to examine non-conscious body size estimation. In this study, AN patients and healthy controls were asked to perform an unrelated task by going through a narrow door. The subconscious extent to which one rotates the shoulders in order to fit through the narrow door was measured (Figure 2). Surprisingly, it was found that AN patients rotated their shoulders more as compared to healthy controls, suggesting that they are non-consciously overestimating their body size [6]. Thus far, both body image components have been shown to exist and more experiments are needed to understand each of their roles in AN etiology.
It is important to distinguish between the perceptual and attitudinal body images, especially for AN etiology because this information is vital to design effective cognitive behavior therapeutic strategies. Often, therapeutic strategies are geared towards modifying the perceptions of AN patients – they are trained to believe that they are not fat [4]. However, the effectiveness of such methods is limited and chances of relapse are high. One study examined if instead of changing the body size perception of AN patients, they can change the definition of thinness and fatness [7]. In other words, can changing the definition of the ‘ideal body’ help in alleviating AN symptoms? Turns out, the answer is yes, it can! AN patients and healthy participants were initially asked to indicate what they thought an ideal body size was, by manually changing the size of a virtual reality avatar. AN patients consistently indicated the boundary between thinness and fatness at much lower body sizes as compared to controls. Subsequently, all participants were taught to modify the boundary, such that the ‘ideal body size’ was 2 sizes higher than the one initially defined by the participants. Indeed, this method was successful in redefining the ‘ideal body size’ in the perception of AN patients, since after training they indicated the new body size to be the ‘ideal body size’. The authors tested the patients for up to a month after training and the training was successful in maintaining the redefined ideal body size. However, the most heartening aspect of this study was that after the redefinition, AN patients reported reduced body dissatisfaction and reduced body size estimation errors, suggesting that this cognitive behavior therapy is effective for AN treatment.
The neural basis of body image distortion
Visual perception
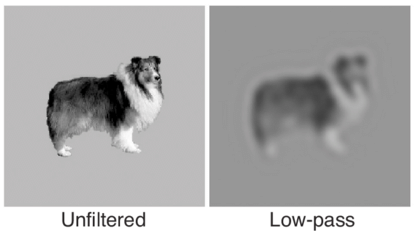
Figure modified from: https://link.springer.com/article/10.3758/BF03206498
Given that AN and BDD are perceptive disorders, it is difficult to model these disorders in genetically tractable laboratory model organisms. However, functional Magnetic Resonance Imaging (fMRI, a scanning technique that measures changes in blood flow related to brain activity) studies on AN patients, AN-recovered and healthy controls have yielded some insight into the brain regions most affected in AN and BDD. One of the brain regions that consistently shows differences among AN / BDD and healthy control groups is in the dorsal (DVS) and ventral visual stream (VVS) which are important regions for processing visual information. DVS is important for integration of visual cues so as to form holistic pictures, particularly when presented with low-stimulus filtered images (for example, low-pass filtered image Figure 3). VVS is important for picking out finer details in an image, typically when visual stimuli are rich in detail (such as the unfiltered image in Figure 3). Across several fMRI studies in AN and BDD patients, it has been found that there is abnormal reduction in activity within the DVS, and an increase in activity in the VVS [8, 9]. This can explain a core symptom of obsession and fixation over minute facial and body features in AN and BDD, while being unable to ‘see’ the body as a whole.
Limbic and cognitive neural circuits
Common comorbidities (simultaneous occurrence of two diseases or conditions) for AN and BDD include anxiety, depression and obsessive compulsive behavior. Indeed, fMRI brain scanning of AN-recovered patients show increased activity in brain regions comprising the limbic system. Brain regions such as the amygdala, ventral side of the anterior cingulate cortex (ACC) and insula, which are important for emotion and mood regulation, could be also regulating the emotional responses to body image stimuli in AN patients. Another neural circuit showing increased activity comprises brain regions important for selective attention processing and planning such as hippocampus, dorsal regions of the ACC and some areas of the prefrontal cortex. It is important to note that the same regions are also observed to be overactive in other psychiatric illnesses like Obsessive Compulsive Disorder, or OCD [10]. These scanning studies are a great start to explain the neural circuitry basis of behavioral characteristics seen in patients with body image distortions.
Concluding remarks
Body image is an important neurobiological and psychological construct, as it forms a visual representation of the ‘self’ in the world, which helps us to analyze daily social interactions and self-behaviors from an objective lens. As much as body image is a personal representation, it is heavily influenced by socio-cultural factors. With the advent of social media, we are all subject to the socio-cultural norms that shape the ‘ideal’ or ‘normal’ body type. There is a constant, intense pressure to look thin in order to be perceived as beautiful, qualified and competent. While eating and body dysmorphic disorders are extreme manifestations of body image distortions, we are all subject to body image issues. You need only evaluate your own relationship with food and exercise in order to understand the impact body image has on self-worth.
Social media frenzy and subsequent craze for Ozempic shows that we are far from being a body positive world. Influencers and celebrities therefore have an important role in spreading the body positivity message, and to be responsible in their messaging about drugs intended for their actual use rather than peddling them for vanity purposes. We live in a self-perpetuating world where we set impossible standards and resort to impossible measures to achieve them. Yet, as the study on modifying the definition of ‘ideal body type’ shows [7], we can achieve true body positivity by changing definitions and behaviors as a society on the whole.
References
Cover picture credits: These ads appear all over the New York City subway station. Click here to learn more.
- Dane A, Bhatia K. The social media diet: A scoping review to investigate the association between social media, body image and eating disorders amongst young people. PLOS Global Public Health. 2023;3: 1–26. doi:10.1371/journal.pgph.0001091.
- Cash TF, Deagle III EA. The nature and extent of body-image disturbances in anorexia nervosa and bulimia nervosa: A meta-analysis. International Journal of Eating Disorders. 1997;22: 107–126. doi:https://doi.org/10.1002/(SICI)1098-108X(199709)22:2<107::AID-EAT1>3.0.CO;2-J.
- Riva G. Out of my real body: cognitive neuroscience meets eating disorders. Frontiers in Human Neuroscience. 2014;8. doi:10.3389/fnhum.2014.00236.
- Cornelissen PL, Tovée MJ. Targeting body image in eating disorders. Current Opinion in Psychology. 2021;41: 71–77. doi:https://doi.org/10.1016/j.copsyc.2021.03.013.
- Provenzano L, Porciello G, Ciccarone S, Lenggenhager B, Tieri G, Marucci M, et al. Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality. Journal of Clinical Medicine. 2020;9. doi:10.3390/jcm9010098.
- Beckmann N, Baumann P, Herpertz S, Trojan J, Diers M. How the unconscious mind controls body movements: Body schema distortion in anorexia nervosa. International Journal of Eating Disorders. 2021;54: 578–586. doi:https://doi.org/10.1002/eat.23451.
- Gledhill LJ, Cornelissen KK, Cornelissen PL, Penton-Voak IS, Munafò MR, Tovée MJ. An interactive training programme to treat body image disturbance. British Journal of Health Psychology. 2017;22: 60–76. doi:https://doi.org/10.1111/bjhp.12217.
- Li W, Arienzo D, Feusner JD. Body Dysmorphic Disorder: Neurobiological Features and an Updated Model. Z Klin Psychol Psychother (Gott). 2013;42: 184–191. doi:10.1026/1616-3443/a000213.
- Moody TD, Morfini F, Cheng G, Sheen CL, Kerr WT, Strober M, et al. Brain activation and connectivity in anorexia nervosa and body dysmorphic disorder when viewing bodies: relationships to clinical symptoms and perception of appearance. Brain Imaging Behav. 2021;15: 1235–1252. doi:10.1007/s11682-020-00323-5.
- Kaye WH, Fudge JL, Paulus M. New insights into symptoms and neurocircuit function of anorexia nervosa. Nature Reviews Neuroscience. 2009;10: 573–584. doi:10.1038/nrn2682.

You must be logged in to post a comment.