 August
18
August
18
Tags
Mind your P’s and T’s: How tainted drugs revolutionized Parkinson’s research
In 1982, a man was brought to a hospital in the Bay Area of California in a curious condition. The man was completely catatonic (immobile), and was frozen into an awkward, statue-like posture. Doctors initially diagnosed him with catatonic schizophrenia, a sub-type of schizophrenia characterized by rigidity and unresponsiveness. However, this diagnosis did not entirely fit. Dr. William Langston was asked to examine the patient and quickly came to the conclusion that the patient – George Carillo – actually had Parkinson’s Disease (PD), and not schizophrenia.
This was a surprising diagnosis. While PD is in part characterized by motor disturbances like tremors and rigidity, it is a progressive disease, meaning that its symptoms slowly worsen over the course of years. Additionally, these symptoms typically emerge around age 60. Mr. Carillo had gone from healthy to catatonic in just a few days and was relatively young. Over the course of a few weeks, five more people that were similarly “frozen” arrived at Bay Area hospitals. Why had six young, healthy people suddenly developed severe PD? Was there something that they all had in common? Little did Dr. Langston know, solving this mystery would transform our understanding of the molecular mechanisms of Parkinson’s Disease.

An example of catatonia
It turned out that all six were heroin users. What is more, they had all acquired their drug from the same exact source. Dr. Langston was able to obtain a sample and sent it out for analysis, which revealed that the “frozen addicts” had not injected heroin as they intended, but had instead injected a synthetic opiate called MPPP (an analog of the opiate painkiller demerol), as well as another unidentified compound. However, MPPP shouldn’t have caused Parkinson’s. Though never marketed, in 1947 Albert Ziering and John Lee had synthesized and tested MPPP on rats, and it appeared to be relatively safe [1]. Thus, the unidentified compound seemed likely to have been the culprit, but since its identity was unknown it was impossible to test its effects.
It was around this time that a friend told Dr. Langston of a remarkably similar case he had encountered in the scientific literature. In 1976, a chemistry student named Barry Kidston abruptly developed PD. Like Dr. Langston’s six patients, Kidston was an opiate user, but unlike them he was also an aspiring chemist. He had read the original 1947 paper by Ziering and Lee and decided to try to synthesize his own MPPP, since it was a completely legal opiate. And he succeeded. He was able to synthesize and use MPPP for several months, until one time he was in a hurry and rushed through the reaction procedure. When he injected the product of this final reaction, he became catatonic. Investigators analyzed his glassware and found MPPP as expected, but also another compound: MPTP. This MPTP impurity had formed because Kidston allowed the reaction mixture to become too hot during his synthesis [2].
When Dr. Langston read this report, he knew he had found something, as he was now able to identify the previously unknown substance as MPTP. Thus, in both of these incidents, opiate users had injected MPTP and then rapidly developed PD, strongly hinting that it was responsible. But Dr. Langston was not the first person to think this. The original investigators into Kidston’s case had tried giving MPTP to rats, but they had been relatively unaffected by it [2]. Still, the circumstantial evidence was strong and drugs sometimes affect different species differently, so Dr. Langston decided to administer MPTP to monkeys. Within just days of injecting MPTP, the monkeys developed Parkinson’s-like symptoms [3]. Dr. Langston at last had his culprit, and would later write a book about his experience entitled: The Case of the Frozen Addicts.
But why and how does MPTP cause PD? It turns out MPTP itself is fairly innocuous, but it is converted by the body into a potent neurotoxin named MPP+. MPP+ kills cells by binding to and disrupting mitochondria. If you remember one thing from high school biology class it is (I hope) that mitochondria are the powerhouse of the cell. When MPP+ binds to mitochondria, it prevents them from providing energy to the cell and also causes them to generate damaging molecules called free radicals. These changes in turn lead to cell death [4].
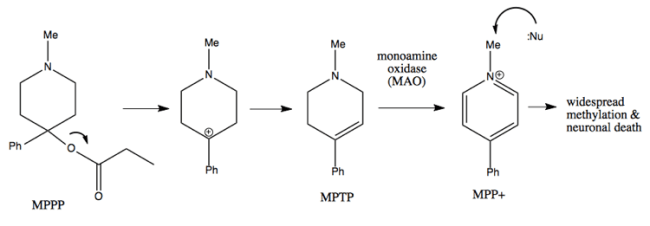
If the reaction is allowed to become too hot during MPPP synthesis, MPTP will be formed. Inside the brain, MPTP is converted by the monoamine oxidase enzyme into the neurotoxin, MPP+.
So MPP+ causes cells to die, but why does this cell death cause PD? First, some background on PD. Although the neurotransmitter dopamine is most often thought of as the brain’s “reward chemical”, it also plays an absolutely crucial role in motor control. Many of the brain’s dopamine neurons are located within the substantia nigra, a brain region that is likewise important for initiating and controlling movement. PD is characterized by massive, progressive cell death of dopamine neurons within the substantia nigra. It is this cell death in the substantia nigra that causes the motor symptoms of PD.
Post-mortem analysis of Barry Kidston’s brain (who died of a drug overdose many months after developing PD) revealed that MPP+ similarly caused dopamine neurons within the substantia nigra to die, indicating that MPP+ was somehow selectively destroying dopamine neurons. One thing that distinguishes dopamine neurons from other types of neurons is that they have the dopamine transporter (DAT) which recycles dopamine from the synapse back into the cell so that it can be re-used. Unfortunately, MPP+ has a chemical structure that is close enough to dopamine that DAT will transport MPP+ as well as dopamine inside the cell. Thus, because MPP+ is only brought inside dopamine neurons, only these neurons die, leading to selective cell death of dopamine neurons within the substantia nigra, just like in PD.
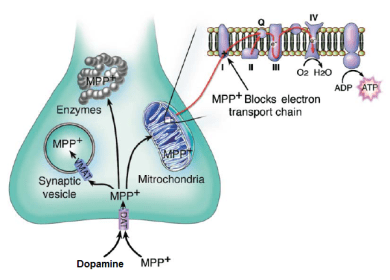
MPP+ and dopamine are transported by the dopamine transporter (DAT) into a neuron. From here, MPP+ disrupts the electron transport chain of mitochondria, preventing them from providing energy to the cell. MPP+ also disrupts the function of various enzymes.
Although the circumstances of the “frozen addicts” were undeniably tragic, there is something of a silver lining. For the individuals themselves, all six responded to typical PD medication. In fact, several of the patients – including the original patient George Carillo – underwent a remarkable treatment: transplantation of fetal dopamine neurons into the brain. A recent follow-up found that these transplants were safe and remarkably effective at reducing some symptoms of PD [5].
On the larger scale, MPTP revolutionized PD research. Though we currently do not know what causes dopamine cell death in PD (see this Neuwrite post by Cailey Bromer for some discussion on pesticides as a possible cause), MPTP allows researchers to model some of the key pathology behind PD. Though other models existed prior to MPTP, it much more closely (though still imperfectly) replicates the pathology and behavioral symptoms of PD. Indeed, researchers have taken this further by developing procedures that combine chronic doses of MPTP with other drugs to, in part, replicate the progressive nature of Parkinson’s [6]. In addition to improving our understanding of PD, these models also allow researchers to develop and test new treatments, aimed to either reduce the symptoms of PD or even prevent the neurons from dying in the first place.

Five of the “frozen addicts”
When asked to help diagnose that first MPTP patient, Dr. Langston could hardly have predicted the remarkable consequences his investigation would have for Parkinson’s Disease research. It is incredible to reflect on the ability of such small, seemingly random events to utterly alter our world. Had MPTP’s neurotoxic effects never been discovered, researchers might still be struggling to create an adequate model of PD. Instead, they now have a way to both investigate the nature of PD and to develop and test novel treatments aimed at improving the lives of the millions of people afflicted with the disease worldwide.
References
- Ziering, A.; Lee, J. (1947). “Piperidine derivatives; 1,3-dialkyl-4-aryl-4-acyloxypiperidines”.The Journal of Organic Chemistry. 12 (6): 911–914. doi:10.1021/jo01170a024.PMID 18919744.
- Davis, G. C., Williams, A. C., Markey, S. P., Ebert, M. H., Caine, E. D., Reichert, C. M., & Kopin, I. J. (1979). Chronic Parkinsonism secondary to intravenous injection of meperidine analogues. Psychiatry Research, 1(3), 249–254.
- Langston, J. W., Forno, L. S., Rebert, C. S., & Irwin, I. (1984). Selective nigral toxicity after systemic administration of 1-methyl-4-phenyl-1,2,5,6-tetrahydropyrine (MPTP) in the squirrel monkey. Brain Research, 292(2), 390–394.
- Dauer, W., & Przedborski, S. (2003). Parkinson’s Disease: Mechanisms and Models. Neuron, 39(6), 889–909. http://doi.org/10.1016/S0896-6273(03)00568-3
- Hallett, P. J., Cooper, O., Sadi, D., Robertson, H., Mendez, I., & Isacson, O. (2014). Long-Term Health of Dopaminergic Neuron Transplants in Parkinson’s Disease Patients. Cell Reports, 7(6), 1755–1761. http://doi.org/10.1016/j.celrep.2014.05.027
- Meredith, G. E., & Rademacher, D. J. (2011). MPTP Mouse Models of Parkinson’s Disease: An Update. Journal of Parkinson’s Disease, 1(1), 19–33. http://doi.org/10.3233/JPD-2011-11023
Images
Featured Image: http://d.gr-assets.com/books/1388804488l/1510265.jpg. Taken From: Langston, J. W.; Palfreman, J. (May 1995). The Case of the Frozen Addicts. Pantheon Books. ISBN 0-679-42465-2.
Image 1: http://www.minddisorders.com/images/gemd_01_img0029.jpg
Image 2: Adapted from [4]: http://doi.org/10.1016/S0896-6273(03)00568-3
Image 3: http://www.cureffi.org/2015/03/04/organic-chemistry-14/
Image 4: https://mmcneuro.files.wordpress.com/2013/12/frozen.jpg?w=315&h=266

{kind=link}
{kind=link}
{kind=link}
You must be logged in to post a comment.