 August
31
August
31
Tags
Psychosurgery: from ice picks to electrodes
If you were to hazard a guess at the date of the first neurosurgery, what would you say?

- An image from [1] showing evidence of brain surgery in a Stone Age skull
I’m going to bet that “the Stone Age” didn’t occur to you as a legitimate answer, but a skeleton dated to roughly 5000 B.C. shows evidence of surgically-created skull holes! While you might be imagining a horribly botched surgery with the patient bleeding out on the table (stone slab?), a closer look at the holes reveals remarkable healing: the skull’s owner lived long after his surgery [1]! We have no real clues as to why our Stone Age surgeon felt that drilling holes in this man’s skull was the right course of treatment. The reason was likely somewhat misguided (e.g. providing an escape route for the evil demons causing his headaches). After all, a famous medical book from 1621 A.D. (~6600 years later!) still called for boring a couple holes in the skull to release the “fuliginous vapors” causing depression, vapors that apparently came from eating too much cabbage [2,3]. (Side note: the book’s full title is, I kid you not, The Anatomy of Melancholy, What it is: With all the Kinds, Causes, Symptomes, Prognostickes, and Several Cures of it. In Three Maine Partitions with their several Sections, Members, and Subsections. Philosophically, Medicinally, Historically, Opened and Cut Up)… #titlegoals.

- A diagram of Moniz’s original leucotomy procedure [2]
While the idea of psychosurgery (neurosurgical treatment for a brain disorder) is an old one, the practice gained popularity starting in the 1930s. Portuguese neurologist Egaz Moniz and neurosurgeon Pedro Almeida Lima used a rod with a retractable wire loop (leucotome) to scoop out a bit of their patients’ frontal lobes [2].
-

- The prefrontal cortex in red
Moniz called the surgery a “leucotomy.” The practice soon gained popularity, at first in Italy and a few years later in the U.S., where it was renamed “lobotomy.” Both terms refer to a surgery that destroys many of the connections to and from the prefrontal cortex, a region known as the hub decision-making, executive thought, personality, etc.
Today, the term lobotomy is irrevocably linked to Dr. Walter Freeman II who pioneered the surgery stateside in 1936. He tinkered with Moniz’s technique and about ten years later adopted a new method from Italian neurosurgeon Amarro Fiamberti: going in through the eye socket with an ice-pick-esque tool (don’t worry, patients were first given electroconvulsive treatment until unconscious) [2]. This particular surgery became known as the transorbital (“through the eye socket”) lobotomy.
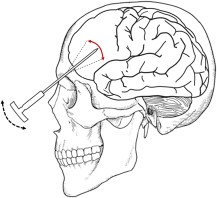
A transorbital lobotomy as popularized by Walter Freeman [2]
How common was the procedure? About 50,000 people in the U.S. received lobotomies, most of them in the late 1940s and early 1950s. Freeman himself performed up to 5,000 lobotomies, once performing 228 in a two-week period in West Virginia!! (In fact, the procedure was so quick and untechnical that Freeman drove around the country doing the surgeries out of a truck that he called his “Lobotomobile.” I imagine it playing the same tune as an ice cream truck.)  Some of his patients reported improvements, some did not experience any change, many were completely incapacitated, and a bunch died. One of his most famous failures is Rosemary Kennedy, an older sister of JFK (a story still crazy enough to make the cover of People decades later!). Rosemary was lobotomized at the age of 23 because of behavioral issues and was so incapacitated by the surgery that she was institutionalized for the rest of her life.
Some of his patients reported improvements, some did not experience any change, many were completely incapacitated, and a bunch died. One of his most famous failures is Rosemary Kennedy, an older sister of JFK (a story still crazy enough to make the cover of People decades later!). Rosemary was lobotomized at the age of 23 because of behavioral issues and was so incapacitated by the surgery that she was institutionalized for the rest of her life.
While now it seems mind-numbingly obvious that the lobotomy was a commercialized, barbaric way to treat mental illness, it gained popularity for one simple reason: there were few alternatives. In fact, Egaz Moniz won a Nobel Prize in 1949 for inventing the procedure, which silenced many contemporary objectors (perhaps unsurprisingly, there is now a movement to rescind the prize). Freeman promoted the procedure as a cure-all, but he blew his success far out of proportion. It was in no way a miracle cure; no one was seriously ill before the procedure and healthy afterwards.

From One Flew Over the Cuckoo’s Nest in which the protagonist is given a lobotomy
How did anyone even begin to perceive the surgery as a success? Sometimes, the procedure did limited damage to a person who was not very ill begin with, and the patient–possibly via placebo effect–reported a positive change in mood without losing cognitive capabilities. In other cases, patients with serious mood disorders exhibited extensively decreased cognitive capacity after the surgery but also diminished agitation. A vegetative state, but at least a calm vegetable? And those were the good outcomes.
The heyday of psychosurgery ended in 1954 with the introduction of the antipsychotic medication chlorpromazine (Thorazine), offering a treatment for mental illness that didn’t involve ice-picks or eye sockets. Despite lower demand for his surgery, Freeman kept right on ice-picking, performing his last transorbital lobotomy in 1967 on Helen Mortensen. She was receiving her third lobotomy from Freeman (now in his 70s) and died from a hemorrhage afterwards. Freeman did not exactly go out on a high note.

- The cingulate gyrus in green
Is psychosurgery still a thing? Yes. Somewhat reminiscent of lobotomies, bilateral cingulotomy is still used as a last resort to treat major depressive disorder and obsessive-compulsive disorder. The surgery involves lesioning the cingulate gyrus, a region that aids in emotional processing and behavioral regulation. However, we’re not talking lesioning in the form of waving an ice-pick around. Today, preliminary MRI scans are taken before the surgery to aid in precise localization of the target region. Using these scans a guide, the surgeon drills a hole in the skull, extends an electrode into the cingulate gyrus, and heats the tip of the electrode to kill the tissue surrounding the electrode tip. Anterior capsulotomy is a similar procedure targeting the anterior portion of the internal capsule and is used to treat obsessive-compulsive disorder [2].
A new(ish), different type of psychosurgery is gaining far more momentum. Deep brain stimulation (DBS) involves surgically implanting a stimulation device into the brain. While there is extensive historical precedence for electrical stimulation as a last-resort psychiatric treatment, DBS in its current form is relatively safe and has been effective in treating a range of neurological disorders, particularly Parkinson’s disease, Tourette’s syndrome, and essential tremor. It will likely soon replace ablative surgery.
Perhaps, years from now, when we have a perfect, effective, totally non-invasive method for treating psychiatric disorders, people will look back on DBS and think we were as crazy as Freeman. At least we’re not doing DBS surgeries out of an ice-cream truck.
References
- Alt KW, Jeunesse C, Buitrago-Téllez CH, Wächter R, Boës E, Pichler SL. Evidence for stone age cranial surgery. Nature. 1997 May 22;387(6631):360. Erratum in: Nature 1997 Jun 19;387(6635):768. PubMed PMID: 9163419.
- Neumaier F, Paterno M, Alpdogan S, Tevoufouet EE, Schneider T, Hescheler J, Albanna W. Surgical Approaches in Psychiatry: A Survey of the World Literature on Psychosurgery. World Neurosurg. 2017 Jan;97:603-634.e8. doi:10.1016/j.wneu.2016.10.008. Epub 2016 Oct 13. Review. PubMed PMID: 27746252.
- Stanley WJ. Burton’s Anatomy of Melancholy.

{kind=link}
You must be logged in to post a comment.