 September
14
September
14
What’s the Deal with Migraines??!!
You’re sitting at your desk, hard at work, and suddenly you see a strange spot of bright light, outlined by a brilliant spectrum of reds and blues, hover over your computer screen. You blink and look around, trying to figure out whether the image is coming from the screen or from outside the window. You then realize that the image is imprinted in the same spot in your visual field—that it’s not out in the world at all, but rather in your brain. Oh no, not again, you think…Thirty minutes later, the side of your head is throbbing, and your vision of the world seems to pulsate with your heartbeat. You feel dizzy, sick to your stomach, and can’t bear to look at the sunlight streaming through your window. You lose all your ability to think clearly, the pain in your head so severe that there’s nothing you can do except take some ibuprofen and wait for it to pass.
There’s no mistaking a migraine. If you’re part of the 15% of the global population that suffers from this complex brain disorder1, chances are that you identify with some aspects of the situation outlined above. Unlike other types of headaches, migraines are more intense, recurring, and last for extended periods of time, sometimes on the order of several days. They also frequently occur in stages, with visual, auditory, or olfactory hallucinations called “auras” sometimes preceding the onset of the pain itself2. About one-third of migraine sufferers experience an aura3, an ominous sign that they are about to experience another migraine.

An artistic depiction of a visual aura experienced before the onset of a migraine.
Who gets Migraines?
Migraines can affect anyone, though their likelihood varies slightly depending on age and gender. People tend to first experience migraines during puberty, and migraines are more common in boys than girls. After puberty the situation flips and more women than men experience migraines. Interestingly, the likelihood of experiencing a migraine is lower during pregnancy and higher during menstruation4. Hormonal fluctuations correlate with the likelihood of suffering from migraines, which has led to the hypothesis that hormones underlie the onset of this disorder.
In addition to fluctuations in hormone levels that occur over the course of months to years, migraine susceptibility also varies on shorter timescales; whether a person will experience a migraine at a given time likely depends on factors in that person’s immediate environment. Many migraine sufferers claim that their migraines are triggered by eating certain foods, by exposure to polluted air, or by changes in the weather5. In addition to environmental factors, migraine likelihood can be affected in the short term by a person’s internal physiology. Physiological changes which underlie stress, hunger, and fatigue are likely to induce migraines or at least contribute to their onset6.
Why are Migraines so Painful?!
There are several theories surrounding the neural underpinnings of migraines7,8,9,10, though a few commonalities exist among them. Most notably, these theories tend to consider migraines a neurovascular disorder, meaning that they originate from problems with the blood vessels in the brain.
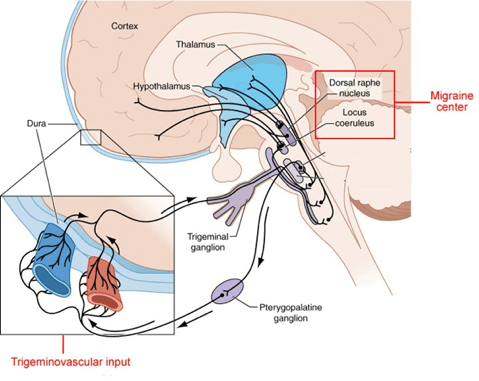
Two anatomical regions that scientists have predominantly put forth as a potential origin of migraines is in deep brain structures and brainstem nuclei. These regions modulate the trigeminovascular system (pictured below) which enables pain and sensory information to be carried between cranial blood vessels and the brain itself11. Interestingly, though, the brain actually doesn’t have pain receptors so the pain sufferers feel when experiencing a migraine isn’t actually their brain that’s hurting! Instead, it’s the adjoining structures such as blood vessels, muscles, and cranial nerves that have pain receptors and therefore “sense” the pain12. When communication between these structures is disrupted, neuronal pain pathways can be activated and a person’s sensory perception can be altered. This leads to symptoms similar to those observed during migraines such as light and sound sensitivity. It’s unclear where the cascade of events begins that results in a migraine, though; some scientists have argued that the trouble starts with the vasculature while others think that the modulation of that vasculature by the brainstem is the culprit.
So, where does this leave us?
Despite the abundance of theories surrounding the physiological disruptions contributing to migraines, studies providing concrete evidence to support these theories are seriously lacking. More research is needed to determine individual susceptibility to experiencing migraines and to devise more effective methods of treatment, since current methods are non-specific to migraines and typically consist of generic pain-relieving medications such as NSAIDs like ibuprofen and naproxen, aspirin, and acetaminophen13. These simple analgesics can be effective for mild to moderate symptoms, but for sufferers of severe migraine pain additional medications are often needed. In addition, pharmacological interventions’ effectiveness can be reduced with frequent use, making medication an unviable option in the long-term. Other than a variety of analgesics, migraine treatment options are few and far between, typically consisting of preventative measures such as stress-reduction, acupuncture, and chiropractic manipulation14,15.
Although they are not life-threatening, migraines cause significant distress and can last from a few hours to three days, dramatically disrupting sufferers’ way of life16. Therefore, we need to continue to explore the mechanisms underlying this disorder if we are to make substantial headway in preventing and treating migraines. Once we more fully understand what changes occur underneath our skull before, during, and after a migraine, we’ll be able to develop a more personalized, precisely targeted, and effective treatment regimen for migraine sufferers.
Sources
- Vos, T; Flaxman, AD; Naghavi, M; Lozano, R; Michaud, C; Ezzati, M; Shibuya, K; Salomon, JA; et al. (Dec 15, 2012). “Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010”. Lancet. 380 (9859): 2163–96. PMID 23245607. doi:10.1016/S0140-6736(12)61729-2.
- Tintinalli, Judith E. (2010). Emergency Medicine: A Comprehensive Study Guide (Emergency Medicine (Tintinalli)). New York: McGraw-Hill Companies. pp. 1116–1117. ISBN 0-07-148480-9.
- Aminoff, Roger P. Simon, David A. Greenberg, Michael J. (2009). Clinical neurology (7 ed.). New York, N.Y: Lange Medical Books/McGraw-Hill. pp. 85–88. ISBN 9780071664332.
- Lay CL, Broner SW (May 2009). “Migraine in women”. Neurologic Clinics. 27 (2): 503–11. PMID 19289228.
- Friedman DI, De ver Dye T (June 2009). “Migraine and the environment”. Headache. 49 (6): 941–52. PMID 19545255. doi:10.1111/j.1526-4610.2009.01443.x.
- Levy D, Strassman AM, Burstein R (June 2009). “A critical view on the role of migraine triggers in the genesis of migraine pain”. Headache. 49(6): 953–7. PMID 19545256. doi:10.1111/j.1526-4610.2009.01444.x.
- Goadsby, PJ (January 2009). “The vascular theory of migraine – a great story wrecked by the facts”. Brain : a journal of neurology. 132 (Pt 1): 6–7. PMID 19098031. doi:10.1093/brain/awn321.
- Brennan, KC; Charles, A (June 2010). “An update on the blood vessel in migraine”. Current Opinion in Neurology. 23 (3): 266–74. PMID 20216215. doi:10.1097/WCO.0b013e32833821c1.
- Dodick, DW (April 2008). “Examining the essence of migraine – is it the blood vessel or the brain? A debate”. Headache. 48 (4): 661–7. PMID 18377395. doi:10.1111/j.1526-4610.2008.01079.x.
- Olesen, J; Burstein, R; Ashina, M; Tfelt-Hansen, P (July 2009). “Origin of pain in migraine: evidence for peripheral sensitization”. Lancet neurology. 8 (7): 679–90. PMID 19539239. doi:10.1016/S1474-4422(09)70090-0.
- Akerman, S; Holland, PR; Goadsby, PJ (2011-09-20). “Diencephalic and brainstem mechanisms in migraine”. Nature Reviews Neuroscience. 12(10): 570–84. PMID 21931334. doi:10.1038/nrn3057.
- Edlow, J.A.; Panagos, P.D.; Godwin, S.A.; Thomas, T.L.; Decker, W.W. (October 2008). “Clinical policy: Critical issues in the evaluation and management of adult patients presenting to the emergency department with acute headache”. Annals of Emergency Medicine. 52 (4): 407–36. PMID 18809105. doi:10.1016/j.annemergmed.2008.07.00.
- Diener, HC; Charles, A; Goadsby, PJ; Holle, D (October 2015). “New therapeutic approaches for the prevention and treatment of migraine.”. The Lancet. Neurology. 14 (10): 1010–22.
- Gilmore, B; Michael, M (2011-02-01). “Treatment of acute migraine headache”. American family physician. 83 (3): 271–80. PMID 21302868.
- Linde, Klaus; Allais, Gianni; Brinkhaus, Benno; Fei, Yutong; Mehring, Michael; Vertosick, Emily A.; Vickers, Andrew; White, Adrian R. (2016-06-28). “Acupuncture for the prevention of episodic migraine”. The Cochrane Database of Systematic Reviews (6): CD001218. ISSN 1469-493X
- Bartleson, JD, Cutrer FM. (2010). Migraine update. Diagnosis and treatment. Minn med 93(5), 36-41.

You must be logged in to post a comment.