 August
22
August
22
Tags
Is evolution the missing link to understanding mental health?
What evolutionary theory can teach us about mental illness
Mental health care has become an increasingly frequent topic in our national dialogue, and with good reason. A 2017 survey reported that nearly 1 in 5 American adults live with a mental illness [1], yet the availability of effective treatment remains scarce. The reasons for this discrepancy are widespread, but from a scientific standpoint, much of the struggle lies in understanding the complex origins of each disorder. The high heritability of most mental illnesses suggests a strong genetic component, but our environment also affects our vulnerability to mental illness (nature and nurture). Scientists and clinicians study both topics in hopes of uncovering how each disorder develops, but some now argue that in order to find better treatments, we also need to understand why these disorders exist. The human brain has been shaped over hundreds of thousands of years, with evolution selecting for traits that helped our species survive and thrive. So why do we still have so many genes that make us struggle? Why did our remarkable cognitive capacity come with such a susceptibility to disorder? The field of evolutionary psychology suggests that looking at mental health from an evolutionary perspective will be critical to addressing our mental health crisis, the same way it has reframed our approach to treating cancer, infections, and metabolic disorders [2]. So what exactly does this evolutionary framework entail?
Many advances in evolutionary medicine begin with the following core concept: bodies are shaped by natural selection to maximize reproductive success, not health or longevity. In the case of cancer, this idea made scientists wonder if we are best at fighting tumors during our reproductive years. They further suggested that instead of trying to destroy a tumor completely, it may actually be better for the body to simply control the damage until the reproductive period is over [3]. This theory could help explain why cancer rates increase with age, while also inspiring new research questions and treatment plans. Instead of using therapies that try to eliminate all cancer cells, we could harness the body’s built-in system for keeping tumors in check. This powerful approach to studying disease is just starting to be applied to illnesses of the brain.
When it comes to mental disorders, there are currently three major theories [4,5] that try to explain why they exist at such high frequencies, despite the fact that many of them reduce a person’s fecundity (how many children you have) [6]. By taking our evolutionary history into account, these ideas aim to make sense of the genetic and environmental causes of mental illness. When we understand how our brains were designed in the first place, we can also learn how best to treat them.
The first theory is the balancing selection hypothesis, where evolution seemingly balances the positive and negative effects of a gene. Genes come in different variations, called alleles, and you have two varieties of every gene (one from each parent). Some alleles increase susceptibility to disorder more than others, but there are several reasons why evolution might have supported the existence of these riskier alleles. For example, you may inherit an allele that is associated with a disease, but is also very useful for other things. A classic example is sickle cell anemia, where having two copies of a particular variant of the hemoglobin gene gives you the disease, but having just one protects you against malaria. In the context of mental health, it’s been suggested that the same alleles that contribute to schizophrenia may have also been integral in supporting human language and creativity [7]. Balancing the costs and benefits of an allele might explain why it continues to be passed on, despite its role in mental illness.
In addition to having different variations of a gene, you can also have multiple copies of it. For example, humans have many more copies of the DUF1220 gene compared to our primate ancestors. The more copies of DUF1220 a primate species has, the larger their brains are [8], which suggests this gene was pretty important to our cognitive evolution. But as it turns out, having more copies of DUF1220 is also associated with increased risk and severity of schizophrenia and autism [9,10].
It’s important to note that not all traits are all-or-nothing; many exist on a continuum where having a moderate amount of the trait is useful, but extremes lead to disorder. This may be an important way of thinking about depression and anxiety, which include some behaviors that are actually helpful when used appropriately. For example, a major symptom in both disorders is rumination, or repetitive thinking. Excessive rumination can make you dwell on negative thoughts or replay unpleasant situations. On the other hand, being able to focus on a problem for an extended period of time can be quite useful for solving it. So this process that creates distress in excess may have initially evolved to support critical thinking and threat management. Even low mood, reduced motivation, and social isolation have been described as evolutionary tools for energy conservation [11]. These traits inform us to change our circumstances (don’t keep doing something that isn’t good for you), and can be used as social signals of defeat to prevent further aggression and encourage others to help. Adopting this sort of view would significantly change our perception of these symptoms, and perhaps even our clinical treatment of them. For example, alternative treatments could support the beneficial aspects of a trait instead of trying to get rid of it completely, i.e. promoting productive analytical thinking in a depressive patient rather than discouraging rumination altogether [11].
A second theory is the environmental mismatch hypothesis, which suggests that a trait may have been good in ancient times, but is detrimental in a modern environment or culture. For example, we know that our ancestors’ ravenous appetite for sugar was useful for maximizing caloric intake when it was hard to come by. But this trait has become quite dangerous now that sugary resources are everywhere. In fact, the same neural pathways that motivated us to seek out these food rewards may have been later co-opted to drive other addictive behaviors. This concept also applies to traits that were previously neutral, but have become problematic as societal demands change. Some psychologists describe dyslexia as a form of neurodiversity that arose from natural differences in neurodevelopment and cognition. It’s our culture’s sudden reliance on written language systems that everyone can conform to that leads these individuals to now be labeled as disordered [12].
This set of ideas may explain some of the nature/nurture interactions that contribute to mental illness, especially since human cultures have been changing much more rapidly in recent history. We have a nervous system that was designed to carry out specific tasks within a tight-knit community, and we are now forcing it to adapt to complex new problems in a social structure that spans the globe. Between our largely sedentary lifestyles, shifting sleep patterns, virtual social interactions, and delayed gratification on increasingly abstract goals, there’s a lot of environmental mismatch to consider.
The third theory is the polygenic mutation-selection balance hypothesis. Unlike the previous two ideas which try to explain why risky alleles are maintained over time, this theory emphasizes that they actually were removed throughout our evolution. The issue is our mental health depends on a very large number of genes, so there are a lot of opportunities for some of them to be risky, and new mutations appear all the time. One study estimated that each human carries ~500 mutations that are bad for brain function [13], but whether or not someone develops a disorder is based on the cumulative effect of their specific combination of mutations. This makes it very difficult to pinpoint the mechanism for each disorder because they develop slightly differently in each person.
There is also growing concern about new mutations appearing at a faster rate than the older ones can be removed. Whenever a reproductive cell (egg or sperm) is made, a new mutation can form and be passed down to a child. The majority of these new mutations come from the father, because more mutations accumulate each time new sperm are made. Since men are often having children later in life, these new mutations are becoming more frequent [14]. Support for the polygenic theory comes from the fact that rarer disorders like schizophrenia and autism have been linked to both newer mutations and increased paternal age [15,16]. On the other hand, more common disorders like depression and anxiety are likely to be evolutionarily older (not caused by random new mutations). Consistent with this idea, they are not as affected by increased paternal age [17].
This theory may be the most accurate and all-encompassing explanation of the genetic forces that contribute to mental illness, but also the hardest to design treatments for. Progress will likely require large numbers of patients to have their whole genomes sequenced in order to find genes worth targeting (a challenging feat).
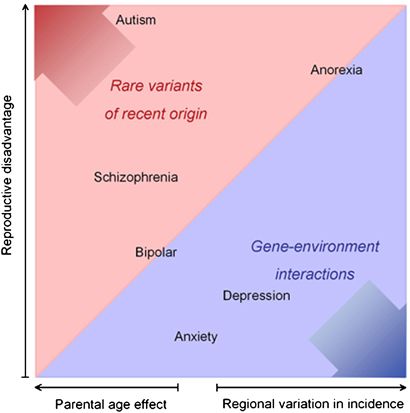
The relative contribution of various factors to different mental disorders. Figure from [4].
These and other ideas will continue to be assessed as we search for the causes of harmful mental illnesses. The reality is likely to be a mix of them all. And yet, despite the useful insights and predictions each theory offers, these concepts are not a part of traditional clinical training, let alone the public perception of mental health. Most clinicians would agree that evolution has shaped the adaptive features of our nervous system, but few take advantage of this perspective when searching for the reasons things can go awry. Adding these ideas to the mix could critically shape the way we conceptualize mental illness in this country. Perhaps we would reevaluate which genes and traits are most important to treat, and develop more effective strategies to do that. Maybe describing these disorders within this larger biological framework provides some comfort to patients whose struggles have been stigmatized. It may also be time to make individual and societal efforts to reduce the modern environmental mismatches that cause us distress. But we can at least be certain that this evolutionary approach will generate new testable hypotheses that reveal a more complete understanding of the origins of mental illness. As a therapy session might suggest, sometimes we have to look back at our past in order to really progress forward.
References:
[1] Substance Abuse and Mental Health Services Administration. (2018). Key substance use and mental health indicators in the United States: Results from the 2017 National Survey on Drug Use and Health (HHS Publication No. SMA 18-5068, NSUDH Series H-53).
[2] Gluckman PD, Low FM, Buklijas T, Hanson MA, Beedle AS. (2011). How evolutionary principles improve the understanding of human health and disease. Evolutionary Applications. 4(2):249–263.
[3] Hochberg ME, Thomas F, Assenat E, Hibner U. (2013). Preventive Evolutionary Medicine of Cancers. Evolutionary Applications. 6(1):134–143.
[4] Uher R. (2009). The role of genetic variation in the causation of mental illness: an evolution-informed framework. Molecular Psychiatry. 14:1072–1082.
[5] Durisko Z, Mulsant BH, McKenzie K, Andrew PW. (2016). Using Evolutionary Theory to Guide Mental Health Research. The Canadian Journal of Psychiatry. 61(3):159–165.
[6] Power RA, Kyaga S, Uher R, et al. (2013). Fecundity of patients with schizophrenia, autism, bipolar disorder, depression, anorexia nervosa, or substance abuse vs their unaffected siblings. JAMA Psychiatry. 70:22–30.
[7] Crow TJ. (1995). Aetiology of schizophrenia: an evolutionary theory. International Clinical Psychopharmacology. 10(3):49–56.
[8] Dumas LJ, O’Bleness MS, Davis JM, et al. (2012). DUF1220-domain copy number implicated in human brain-size pathology and evolution. American Journal of Human Genetics. 91:444–454.
[9] Quick VBS, Davis JM, Olincy A, Sikela JM (2015). DUF1220 copy number is associated with schizophrenia risk and severity: implications for understanding autism and schizophrenia as related diseases. Translational Psychiatry 5: e697.
[10] Davis, JM, Searles VB, Anderson N, et al. (2014). DUF1220 dosage is linearly associated with increasing severity of the three primary symptoms of autism. PLoS Genet, 10: e1004241.
[11] Durisko Z, Mulsant B, Andrews P. (2015). An adaptationist perspective on the etiology of depression. Journal of Affective Disorders. 172:315–323.
[12] Protopapas A and Parrila R. (2018). Is Dyslexia a Brain Disorder? Brain Sciences. 8(4):61.
[13] Keller MC and Miller G. (2006). Resolving the paradox of common, harmful, heritable mental disorders: which evolutionary genetic models work best? Behavioral and Brain Sciences. 29:385–404.
[14] Crow JF. (1999). Spontaneous mutation in man. Mutation Research. 437(1):5–9.
[15] Reichenberg A, Gross R, Weiser M, Bresnahan M, Silverman J, Harlap S et al. (2006). Advancing paternal age and autism. Archives of General Psychiatry. 63:1026–1032.
[16] Malaspina D, Corcoran C, Fahim C, Berman A, Harkavy-Friedman J, Yale S et al. (2002). Paternal age and sporadic schizophrenia: evidence for de novo mutations. American Journal of Medical Genetics. 114:299–303.
[17] Laursen TM, Munk-Olsen T, Nordentoft M, Bo MP. (2007). A comparison of selected risk factors for unipolar depressive disorder, bipolar affective disorder, schizoaffective disorder, and schizophrenia from a Danish population-based cohort. Journal of Clinical Psychiatry. 68:1673–1681.

You must be logged in to post a comment.