 February
27
February
27
Buried Alive
You wake up. It’s pitch black, the air is stale, and your body is pressed by wooden planks on all sides. You try to reach up but your hand hits wooden planks above you. Seized by terror, you try to thrash about but there is no room to move and it’s getting harder to breathe. Your hands hit, scratch, claw at the wood in front of them but nothing moves. With your last gasps of air you scream but the wood and dirt surrounding you swallows the sound.
This scenario was a reality for a disturbingly high number of people only a century or two ago, before good practices and techniques for identifying when a patient was dead became readily available. The podcast Memory Palace tells stories of digging up coffins to find evidence of people who died in the exact scenario described above. One woman tried to claw her way out, ripping her fingernails out in the wood. Another man shattered his skull trying to bash his way out. Not every story ends horrifically; there are stories of dead people waking up at funerals and the resulting mass hysteria this caused. Doctors simply did not have instruments sensitive enough to detect the difference between some reversible conditions (such as comas, epileptic fits, and drug-induced narcolepsy) and actual death.
Though today we are better at determining when ‘vital bodily functions have ceased’—the official medical definition of death—as a society we are still working on our sense of how to define when a brain has ceased to function. The cases of Terri Schiavo & Jahi McMath provide poignant examples of spouses and parents wrestling with the idea of when to declare a loved one dead in the face of impaired brain function. When machines can feed and/or keep someone’s lungs full of air far beyond when their bodies would have failed naturally, the idea of giving up on someone who may still have a fighting chance is hard. To many people, a rising and falling chest and a beating heart are the definition of life. How do we know if we are or are not giving up too early on people with brain damage? What if our measurement tools about brain function are too imprecise? The medical community and scientists have been clarifying the answer to these questions of how to deal with long-term unresponsive patients.
Evidence for conscious thought in the absence of behavior
Sudden brain damage or longer-term degeneration can cause a coma, which is defined as unconsciousness that lasts for greater than 6 hours and a failure to behaviorally respond to external stimuli such as pain, light, or sound (1). Some coma patients recover consciousness and others die from indirectly-related complications (like pneumonia); another subset of coma patients enter into a ‘persistent vegetative state’ which involves a lack of awareness or behavioral response to surroundings but with intact autonomic functions such as a sleep/wake cycle and breathing. Defining the spectrum from patients who are ‘brain dead’ to patients likely to regain consciousness is a still developing field (2). There are a variety of behavioral tests, such as the Moscow Coma Scale, which are used to examine the spectrum of responsiveness to the outside world. Some patients are almost entirely unresponsive (persistent vegetative state) while others show intermittent bouts of behavioral responsiveness (a minimally responsive state). For a review of medicine’s diagnostic criteria see citation 2. Advanced neuroimaging tools offers a complementary view into the brains of these patients to see what the brain is doing when the patient is not obviously responsive.
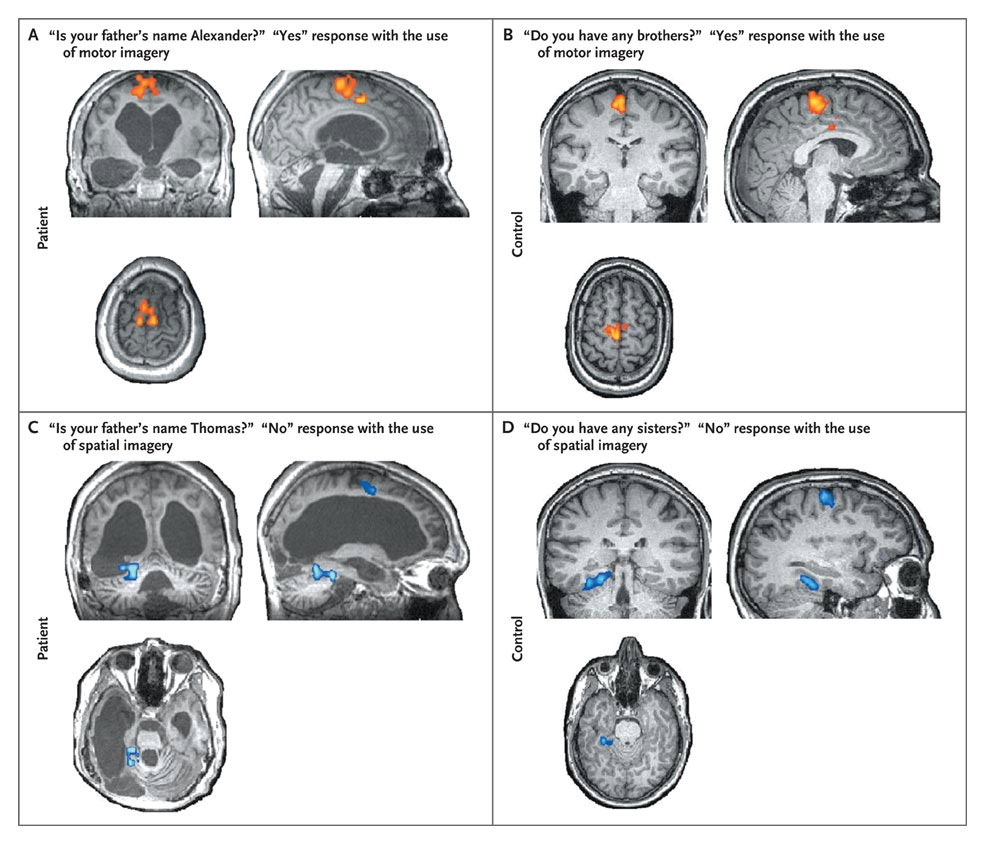
Figure 1. fMRI brain activation maps for a patient (A & C) and control participant (B & D) for a task that asked them to answer yes/no questions by imagining either a motor response (A & B) or spatial response (C & D). Initially, patients and controls underwent a task that asked them to imagine themselves either playing tennis (motor) or navigating the streets of their city (spatial map). During the question portion of the task participants would respond yes or no to questions by using the same type of imagining.
Several novel paradigms have been used to assess whether patients are capable of higher-level brain activity. In one, patients were verbally instructed to imagine either playing tennis (motor-related imagery) or moving around their house (spatial-related imagery), and brain activation was observed using fMRI. The pattern of activity in response to the imagine command in some patients matched the pattern later observed when healthy controls were given the same instructions (3). In another study, 5 out of 54 unresponsive or minimally responsive patients were able to modulate brain activity in response to the imagine commands. Of the 5 patients whose brain was responsive, 2 had not had any responsiveness detected using behavioral methods alone. Further, 1 these patients was claimed to be able to answer yes/no questions with changes in brain activation (4; Figure 1). No communication could be formed with this patient at their bedside. Another study, using electroencephalography, found minimally responsive patients with the neural ability to detect rare sounds (such as their name) among a stream of other sounds (5). Neural tests like these could be of use in distinguishing between subjects who are minimally responsive, and who may have better prognoses, and vegetative patients, who may have worse prognoses. Further, these tests act as evidence that people who are behaviorally unresponsive or have very limited behavioral responses may continue to be able to perform relatively complex cognitive tasks.
There is also the question of whether there are courses of treatment could improve the outcome of these patients. Currently, the course of most treatments is very passive: keep the patient alive and wait for them to die or regain consciousness, but not to try and improve brain function. Would it be possible to develop drugs or techniques to increase the functioning of these patients? Several studies have attempted to use drugs to improve the patients’ outcome. In one, methylphenidate (a stimulant drug used to treat attention deficit disorder) caused an increase in bloodflow in key brain areas correlated with increased behavioral responsiveness (6). A second study found a similar effect with amantadine (an antiviral drug sometimes used for Parkinson’s disease; 7). Another approach is deep brain stimulation, which sends electrodes into the subject’s thalamus (or nearby structures) to deliver electrical charges. A study attempted this therapy on a patient who had not communicated, fed himself, or coordinated movement for 6 years. While this patient was not fully brought back to consciousness, the therapy markedly increased behavioral and neural measures of consciousness (8). None of these treatments has resulted in a patient’s complete recovery, but with a better understanding of which patients to target for treatment, future research may find more effective novel therapies for these conditions.
Brain Death
In some cases of brain damage however, there is no hope for the patient. How do medical professionals distinguish patients that have a fighting chance from those whose brains have ceased to function forever? In the United States since 1997, death has been defined as the irreversible cessation of circulatory and respiratory function OR the irreversible cessation of brain function, particularly the brain stem (which is intimately involved in regulating the basic functions which keep you alive) (9). The reason that brain death is such an important concept is that it allows the removal of life support and/or the beginning of organ donation. As you can imagine, it is critical to have a rigid definition of what constitutes brain death to avoid mistaking a potentially reversible condition that should receive treatment from a case where there is no hope for recovery. A study in 1989 (8 years before the official law on brain death was passed) surveyed 195 medical professionals involved in the process of organ retrieval for transplant, and found that only ~1/3 could correctly identify the legal & medical criteria that defined being brain dead and ~1/5 would classify individuals in a persistent vegetative state as dead (though this is a complex issue, as some patients in persistent vegetative states do not meet the criteria for being brain dead, but are extremely unlikely to ever regain consciousness) (10).
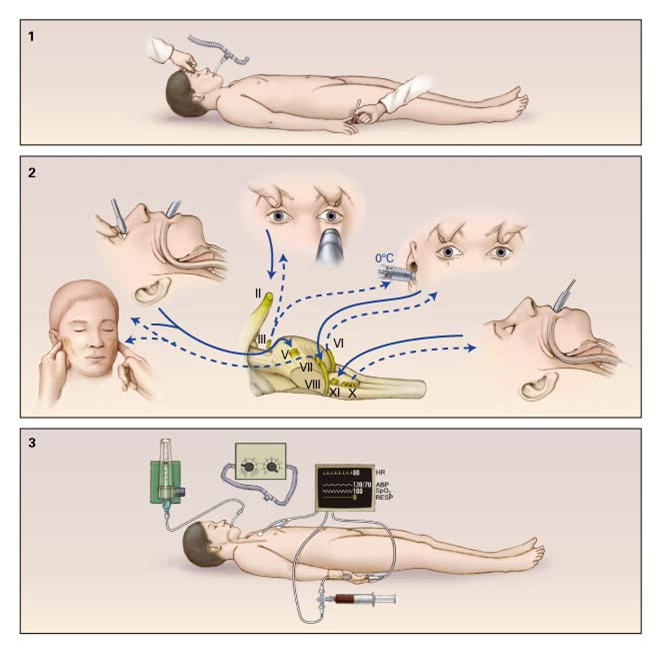
Figure 2. The three-step process to declare someone brain dead in the U.S. 1) Use painful stimuli to test the overall responsiveness of the individual. 2) If no responsiveness is found, test the cranial nerves to test the degree of function in the brain stem. 3) If the brain-stem is non-responsive, test the ability of the brain to sustain self-breathing. If the patient fails all 3 tests, they can be declared brain dead.
The evolving definition of what it means to be brain dead can be traced back to 1959 when 23 patients were declared to have irreversible comas based on the lack of brainstem reflexes, lack of self respiration, and a lack of electroencephalogram activity (a measure of brain electrical activity) (11). There were various revisions to these criteria over the years, particularly the centering of attention on damage to the brain stem (12). Worldwide, differences exist between the specific implementation of the standards necessary to declare someone brain dead but there is broad overall agreement about the general standards for what constitutes ‘brain death’ (13).
In the U.S., here is how you would be declared brain dead. First, it is important to document the causes of the coma (several conditions may mimic brain death such as locked-in syndrome, hypothermia, or drug intoxication). Next, the doctor would perform an examination as shown in Figure 2 (14). First, the depth of the coma is ascertained by examining responses to painful stimuli. If someone is non-responsive to several painful stimuli (such as sticking a pin underneath the fingernail) then the brain-stem responses would be tested. The reasoning is that these reflexes are automatic and governed by a functioning brain-stem, therefore an absence of these reflexes would be proof for severe and irreversible damage to this area of the brain. Since the brain stem is critical to maintaining several processes for life, including breathing, a non-functioning brain stem is a clear indication that the patient cannot recover. Finally, the inability of the brain to sustain life is confirmed through apnea tests. These are designed to test the most basic breathing function of the brainstem: a breath response to high levels of carbon dioxide in the blood. If the brainstem cannot accomplish this, this is strong confirmation the brain can no longer sustain the most basic of life support functions.
Depending on the resources available to the doctor and the medical standards of the country, certain additional tests may confirm the findings of the 3 tests mentioned above. These include tests of blood flow to the brain such as cerebral angiography, transcranial doppler ultrasonography, and positron emission tomography. Another form of testing is the electrical activity in the brain through electroencephalography (mentioned in the original definition of brain death). It is not common to use fMRI to test brain function in a clinical setting as of yet, but perhaps in the future this will also be used. Encouragingly, as of 2010 there are no published cases of misdiagnosing a patient as brain dead only to have them recover neurologic function (15).
Conclusion
We have come a long way in determining medically when critical organs such as the heart have irreversibly ceased to function. Even for the brain, the global medical community has spent the last 5 decades effectively identifying patients whose brains can no longer support life. But for patients in a persistent vegetative state or a minimally conscious state, in the age of ventilators and other future life-support innovations the picture is much less clear. It is tempting to leave the decision of life support in these cases to the broader culture & religions. Deciding when life has ceased even though the heart still beats is a tangled and painful issue because a decision has to be made about continuing or stopping care. People write into their wills (or the equivalent medical document, called an “advanced directive”) to remove them from life support in order to spare their loved ones the decision, since our current medical practices cannot always answer this question conclusively.
But medicine and science are working hard to find evidence that can better inform this weighty decision. Neuroimaging is showing that a subset of patients in a vegetative state have somewhat preserved brain function. Tracking the trajectories of all the subsets of patients will help the medically community to know better what to expect in each patient’s case. Identifying and targeting novel therapies, and understanding the likely trajectory for each patient will help determine which option to choose for each specific case. With additional research, perhaps in the future there will be no question about the decision to remove or not remove someone in a persistent vegetative state from life support.
References
Title picture from the website Lifehacker (http://lifehacker.com/5933568/how-much-sleep-do-you-really-need-to-work-productively)
1) Bordini, A. L., Luiz, T. F., Fernandes, M., Arruda, W. O., & Teive, H. A. (2010). Coma scales: a historical review. Arquivos de neuro-psiquiatria, 68(6), 930-937.
2) Giacino, J. T., Ashwal, S., Childs, N., Cranford, R., Jennett, B., Katz, D. I., … & Zasler, N. D. (2002). The minimally conscious state definition and diagnostic criteria. Neurology, 58(3), 349-353.
3) Owen, A. M., Coleman, M. R., Boly, M., Davis, M. H., Laureys, S., & Pickard, J. D. (2006). Detecting awareness in the vegetative state. Science, 313(5792), 1402-1402.
4) Monti, M. M., Vanhaudenhuyse, A., Coleman, M. R., Boly, M., Pickard, J. D., Tshibanda, L., … & Laureys, S. (2010). Willful modulation of brain activity in disorders of consciousness. New England Journal of Medicine, 362(7), 579-589.
5) Schnakers, C., Perrin, F., Schabus, M., Majerus, S., Ledoux, D., Damas, P., … & Laureys, S. (2008). Voluntary brain processing in disorders of consciousness. Neurology, 71(20), 1614-1620.
6) Kim, Y. W., Shin, J. C., & An, Y. S. (2009). Effects of methylphenidate on cerebral glucose metabolism in patients with impaired consciousness after acquired brain injury. Clinical neuropharmacology, 32(6), 335-339.
7) Schnakers, C., Hustinx, R., Vandewalle, G., Majerus, S., Moonen, G., Boly, M., … & Laureys, S. (2008). Measuring the effect of amantadine in chronic anoxic minimally conscious state. Journal of Neurology, Neurosurgery & Psychiatry, 79(2), 225-227.
8) Schiff, N. D., Giacino, J. T., Kalmar, K., Victor, J. D., Baker, K., Gerber, M., … & Rezai, A. R. (2007). Behavioural improvements with thalamic stimulation after severe traumatic brain injury. Nature, 448(7153), 600-603.
9) Uniform Determination of Death Act, 12 Uniform Laws Annotated (U.L.A.) 589 (West 1993 and West Supp. 1997).
10) Youngner, S. J., Landefeld, C. S., Coulton, C. J., Juknialis, B. W., & Leary, M. (1989). Brain death and organ retrieval: a cross-sectional survey of knowledge and concepts among health professionals. Jama, 261(15), 2205-2210.
11) Mollaret P, Goulon M. Le coma dépassé (mémoire préliminaire). Rev Neurol (Paris)1959;101:3-5
12) Diagnosis of brain death: statement issued by the honorary secretary of the Conference of Medical Royal Colleges and their Faculties in the United Kingdom on 11 October 1976.BMJ 1976;2:1187-1188
13) Wijdicks, E. F. (2002). Brain death worldwide Accepted fact but no global consensus in diagnostic criteria. Neurology, 58(1), 20-25.
14) Wijdicks, E. F. (2001). The diagnosis of brain death. New England Journal of Medicine, 344(16), 1215-1221.
15) Wijdicks, E. F., Varelas, P. N., Gronseth, G. S., & Greer, D. M. (2010). Evidence-based guideline update: Determining brain death in adults Report of the Quality Standards Subcommittee of the American Academy of Neurology.Neurology, 74(23), 1911-1918.

Pingback: Locked In Syndrome: Facing My Nightmare | NeuWrite San Diego