 June
16
June
16
Tags
Breathe in the Benefits: Hyperbaric Oxygen for PTSD
Even if you haven’t heard the term “hyperbaric oxygen treatment” (HBOT), you are actually probably familiar with its premise. Most often, we hear of this treatment being used for divers that ascend from depth too quickly and experience decompression sickness (“the bends”) caused by a buildup of gas bubbles in their blood from rapid changes in the pressure around them. Hyperbaric oxygen therapy involves exposing patients to 100% oxygen at a pressure that is higher than normal atmospheric pressure (“hyper-” meaning over or exceeding, “baric” referring to pressure), usually in specialized chambers built for one person or even rooms that can house multiple patients. For the divers, this reverts them to the pressure they experienced underwater and reverses the bubble buildup until they can be safely and slowly brought back to regular atmospheric pressure.
HBOT in the clinic
Outside of diving, HBOT is surprisingly also used to treat a host of medical maladies, such as infections, burns, wounds that won’t heal, and carbon monoxide poisoning. This is because supplying oxygen at two to three times the normal pressure allows moreoxygen to enter the bloodstream, and then tissues all over the body, as compared to breathing 100% oxygen in a normal room. Having extra oxygen in the bloodstream to supply to our cells supports their critical functions. According to the Mayo Clinic, the increased oxygen also helps fight bacteria and stimulates the release of certain proteins in our cells that promote healing.

More specifically to the brain, HBOT is also used to treat ailments that cause structural damage to brain tissue, such as stroke and traumatic brain injury (TBI). The damage to the blood vessels in the brain that results from these injuries induces a lack of oxygen in the directly damaged and surrounding tissue, which can lead to even more loss of blood vessels as well as decreased activity in neurons and brain support cells that dampens their function. Neurons that don’t receive enough oxygen cannot form or support existing connections with other neurons, which is essential to overall brain function. Additionally, injury to brain tissue, as with the rest of the body, causes inflammation that is initially protective, but overall results in damage that can kill nearby cells and prevent normal activity in the damaged brain area. Studies in both animals and humans suggest that HBOT can be used to treat this direct brain damage by forcing oxygen back into the oxygen-deprived tissue to mitigate all of these detrimental side effects. The enhanced oxygen increases the production of blood vessels, prevents cell death, supports neurons to perform their normal functions and form connections with other neurons, and reduces inflammation [1-4].
Recently, HBOT hit the headlines again with promise for treating a new illness: post-traumatic stress disorder (PTSD). Was hyperbaric oxygen effective in treating patients with PTSD? And how might HBOT and the resulting changes in oxygen work to treat a disorder that we usually attribute to mental dysfunction instead of physical trauma to the brain?
PTSD, Behavior, and the Brain
PTSD is a complicated disorder, but at its basis is defined by the inability to recover fully from a past experienced trauma. Patients with PTSD may find themselves reliving the memories and avoiding places or situations that may bring up memories of that trauma. Certain behavioral symptoms often accompany these experiences, such as the recurrence of angry outbursts and difficulty sleeping, as well as cognitive symptoms like loss of interest in activities and feelings of guilt. PTSD is typically treated by medication or psychotherapy [5].
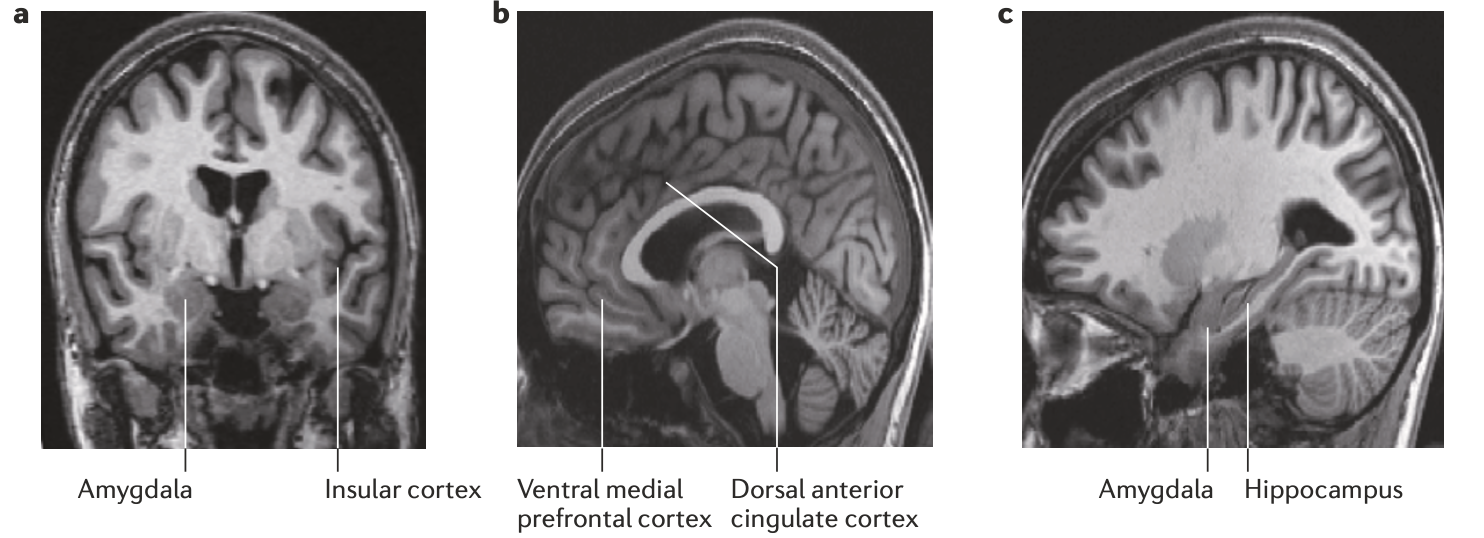
More recently, neuroimaging in humans [6] has uncovered some notable changes in the structure and function of the brains of patients experiencing PTSD. Structurally, PTSD is correlated with smaller volume of the hippocampus (the memory center of our brain) and the prefrontal cortex (a region right at the very front of our brain that is involved in “executive functions,” like planning and decision making). There are noted issues in the quality of the nerve bundles that send information from another area of the cortex (the anterior cingulate cortex, or ACC, which is involved in pain perception and the learning of fearful stimuli) to the amygdala (our brain’s major fear center that recognizes fearful situations and coordinates our response to fear).
In addition to using imaging to look at the structure of the brain, neuroscientists can also use different types of brain scans to determine which regions are active during a particular task. These scans in PTSD patients reveal changes in the level of brain activity in many of the same brain areas as above. The amygdala and ACC increase their activity in a way that correlates with PTSD severity, whereas prefrontal cortex activity decreases. The hippocampus of PTSD patients appears to sometimes increase and sometimes decrease in its activity compared to control subjects depending on the type of task the person is performing during the imaging session. Although there are a lot of brain areas here to keep up with, the basic results of brain imaging in humans with PTSD follow their symptoms: the brain areas related to perception of and response to fear (amygdala and ACC) go into overdrive, while the region that usually functions to keep control over the subconscious drives of the others (prefrontal cortex) is taken offline, resulting in an inappropriate response to fear and stress. Memory is affected in both directions, perhaps leading to the strengthening of fearful memories and the inability to forget the fear and use memories more updated to the current situation.
HBOT for PTSD
Given our current understanding of PTSD symptoms and effects on the brain, a 2022 study from researchers in Israel [7] endeavored to determine whether HBOT could benefit veterans with PTSD that weren’t responsive to the usual treatment options by investigating both their symptoms and the structure and activity in their brains before and after HBOT treatment. Importantly, this publication followed up on a series of papers which indicated that HBOT can relieve symptoms of PTSD in veterans suffering from TBI. While those studies found that HBOT improved the patients’ PTSD symptoms, it was unclear whether the treatment had an effect on PTSD directly or whether the improved PTSD symptoms were a secondary effect of treating the TBI. Therefore, these authors selected patients that experienced PTSD in the absence of traumatic brain injury. Half of the patients were assigned to the treatment group that received HBOT and the other half were assigned to the control group and didn’t receive any additional treatment – both groups continued the therapy and medications they were already taking before the study throughout.
PTSD symptoms in each patient before and after treatment were assessed using a variety of interviews and questionnaires that allowed researchers to give patients an overall score of PTSD severity. While the HBOT and control groups had identical scores before the treatment, the severity of the scores decreased in the HBOT group after three months of treatment for five days each week, whereas control patients saw no improvement in that same time frame. Interestingly, the authors noted that the patients undergoing HBOT experienced a gradual resurfacing of memories related to their trauma, which, in the moment, was extremely distressing. However, this distress was followed by its resolution and integration of the new memory, perhaps contributing to improved PTSD symptoms. These results indicate that repeated HBOT can relieve the behavioral and psychological symptoms of PTSD.
Using a neuroimaging technique that looks at the structure of the brain in detail, researchers found that the brains of patients undergoing HBOT had improved connections in the fiber bundles that transmit activity from the thalamus (the sensory and motor switchboard of the brain) to the frontal lobe of the cerebral cortex, one part of which is the “executive” prefrontal cortex. They also noted better connections between the two sides of the frontal cortex on each hemisphere of the brain. When the patients were assessed using a different type of scan that pinpoints areas of activity in the brain, the researchers found improved activity in the prefrontal cortex, the thalamus, and the hippocampus (the memory center), along with other cortical areas serving a variety of functions. These results are important because a breakdown in the activity of and communication between the executive, memory, and emotional parts of the brain are known to correlate with severe PTSD symptoms, such as emotional dysregulation and the inability to inhibit emotional outbursts. Therefore, an improvement in brain signaling in those areas could explain the improved PTSD scores in HBOT patients. As previously discussed, the hippocampus also plays an important role in PTSD, and its breakdown may result in the memory deficits, information processing issues, and inability to extinguish the fear that PTSD patients experience. Improved hippocampal activity in the veterans studied here could also help explain the overall PTSD symptom improvement after HBOT therapy.
While this study produced interesting results that could suggest future applications for HBOT in the treatment of PTSD, there are some important caveats to bear in mind when assessing the results. First, the authors note that this study relied on only a small number of individuals (about 15 patients in each of the HBOT and control groups). Additionally, as being in the presence of hyperbaric oxygen is pretty obvious, the researchers opted not to have a “sham” condition in which their control patients participated in a similar therapy that wasn’t actually a high pressure,100% oxygen environment. Because of this, it is difficult to parse out how much of the success achieved in the patients was due to HBOT versus the placebo effect. The patients undergoing HBOT were participating in a new therapy and inherently received more attention from medical professionals compared to the control group going about their usual therapies. The expectation of symptom improvement in these conditions can often lead to actual symptom improvement. Finally, it is not exactly clear how the increased brain oxygenation provided by HBOT improved the function of the same brain areas implicated in PTSD in the absence of major tissue damage.

HBOT for future mental health applications?
Despite the caveats in the above study, HBOT certainly may represent an interesting, non-invasive avenue for the future treatment of PTSD and other mental health disorders in conjunction with behavioral therapy and pharmaceutical treatment. While an internet search for HBOT in depression, anxiety, addiction, and the like reveals many company websites that tout the benefits of their hyperbaric treatment in these disorders, neuroscientists are just beginning to determine the effectiveness of the treatment in the absence of brain tissue damage. Future studies in the field are necessary to determine the mechanisms by which we may be able to heal dysregulated activity in the brain to support mental health.
References
- Efrati S, Ben-Jacob E (2014) Reflections on the neurotherapeutic effects of hyperbaric oxygen. Expert Review of Neurotherapeutics, 14(3):233-236
- Huang L, Obenaus A (2011) Hyperbaric oxygen therapy for traumatic brain injury. Medical Gas Research, 1:21
- Zhang JH, Lo T, Mychaskiw G, Colohan A (2005) Mechanisms of hyperbaric oxygen and neuroprotection in stroke. Pathophysiology, 12:65-80
- Lin KC, Niu KC, Tsai KJ, Kuo JR, Wang LC, Chio CC, Chang CP (2011) Attenuating inflammation but stimulating both angiogenesis and neurogenesis using hyperbaric oxygen in rats with traumatic brain injury. Journal of Trauma and Acute Care Surgery, 72(3): 650-659
- National Institute of Mental Health (2019). Post-traumatic stress disorder. Retrieved June 13, 2022, from https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd.
- Pitman RK, Rasmusson AM, Koenen KC, Shin LM, Orr SP, Gilbertson MW, Milad MR, Liberzon I (2012) Biological studies of post-traumatic stress disorder. Nature Reviews: Neuroscience, 13: 769-787
- Doenyas-Barak K, Catalogna M, Kutz I, Levi G, Hadanny A, Tal S, Daphna-Tekoha S, Sasson E, Shechter Y, Efrati S (2022) Hyperbaric oxygen therapy improves symptoms, brain’s microstructure and functionality in veterans with treatment resistant post-traumatic stress disorder: A prospective, randomized, controlled trial. PLoS ONE, 17(2):e0264161
Cover Image Source: BokicaK/Wikimedia Commons/GFDL 1.2

You must be logged in to post a comment.