 December
31
December
31
Life After Death(?): From Strokes to Sci-Fi
Death is not a singular event, as implied when we refer to the “time of death” or “moment of death”. It is a relatively long, drawn out, active process: these terms merely simplify and provide a hard boundary. Not everything in the brain (or the rest of the body) dies at the same time, at the same rate. Outside of traumatic events, nearly all necrotic (arising from external factors, rather than being programmed) cell death in the brain arises from “ischemia”, the loss of a constant oxygen supply, which in most cases itself arises from loss of blood flow [1]. Loss of oxygen doesn’t just kill cells instantly once cut off from supply. Instead, cell death is prolonged, arising from destabilization of internal functions reliant on oxygen. For example, most methods of energy generation in the cell require oxygen, and without it, cells either switch to less efficient methods (which do not produce enough energy alone to power the cell), or they continue producing energy the same way while damaging the biological machinery required to do it. Eventually, both kill the cell. Crucially, however, these operate on a relatively long delay: even though normal neurological function shuts down, some cells take hours or even days to die afterwards [2].
In fact, many techniques in neuroscience exploit “incomplete” death in the brain to examine its function. The most common is electrophysiology, the process by which neuroscientists can record electrical activity in individual neurons. The procedure requires removal of tissue from the brain shortly after death, but the whole brain cannot be dead: you can only record from live cells, which are preserved by immediately replacing blood with ice-cold, optimized, oxygenated solutions [3]. Physiologists then find and record from live cells within the “dead” tissue, taking advantage of the fact that some cells stay alive for a relatively long period. In fact, methods to euthanize animals while keeping brain cells as viable as possible for as long (up to 12 hours in mice, and 60 in humans!) as possible constitutes a highly active subfield of research [4]. These researchers aim to alter the parameters of death to keep neurons living longer externally in as close to normal conditions as possible, manipulating the boundary between life and death on the margins.
Out in the Cold
However, these are simply single cells. Can we exploit this delay in whole tissues as well? In fact, this is exactly what enables treatment and recovery from strokes, which are at base just local interruptions to blood supply caused by blood clots. If cells within a tissue die in minutes following ischemia, strokes would be nigh impossible to treat. Instead, strokes have a window for treatment known as the “golden hour”, where many patients can recover if given anti-clotting drugs within this window [5]. Recently, though, researchers have been able to use imaging methods to identify tissue with the highest likelihood of recovery. Such practices are allowing us to open this extremely narrow window further, first up to 4.5 hours, and now even up to 16 in some specific cases [6,7]. These methods mostly focus on identifying and prioritizing the tissue with the highest chance of survival, along with more “traditional” advances like more effective drug compounds and formulations. Like electrophysiology, these methods constitute an extremely active field of research with continuously advancing practices, but these advances are even now having a real effect on stroke care, pushing the frontier of treatment forward.

Okay, then what about whole bodies and whole brains? Perhaps unsurprisingly, we can also now restore larger-scale tissues from severe, otherwise lethal damage (albeit under very specific conditions), returning them to usable condition despite dramatic trauma. One of the first well-studied cases occurred in 1999, when Anna Bågenholm, a Swedish doctor, lost control while skiing [8]. She fell and became wedged between rocks and ice for more than an hour and a half, while her body temperature dropped to 57 degrees F (the norm is 98.6), and lost all signs of life, appearing clinically “dead.” Like in electrophysiology, the key to her survival was that she was quite literally ice-cold. Doctors were able to remove her blood from her body, circulate it through warm tubes in a bypass heater, and then return the blood to the body, but now at normal body temperature. After 9 hours, she was returned to a normal temperature and resuscitated. She took almost two months to return from the hospital, with many complications like partial paralysis and weakness, but she was alive.
As these methods have been refined further, so has our ability to treat these cases. In 2006, an anonymous 17-year-old girl was found in a field with severe hypothermia with a very weak pulse and a core body temperature of 65 degrees F [9]. She was brought to the emergency room, and in transit, her heart completely stopped. Doctors treated her like they did Bågenholm, circulating her blood in a heater, and then returning it to the body warmed to body temperature [9]. However, resuscitation now took under 4 hours, and 11 days later, she left the hospital as if nothing had happened, with full function restored in a fraction of the time. As a result of such incidents, a new phrase has become increasingly common in emergency medicine: “You’re only dead once you’re warm and dead.”
Into the Future
All of these developments in methods have led to a single point, which synthesized all of these advancements together, from electrophysiological solutions, to cold preservation, to post-mortem intervals: the brain in a vat. This study has actually been discussed in far greater detail at NeuWrite SD, both in terms of its wider ethical implications and the actual details of the study itself previously, so go check out those posts! In short, researchers were able to extract brains from pigs up to 4 hours after death, and then keep them alive for up to 6 hours after preservation began [10]. Neurons in these brains remained viable, with preservation of metabolism, reductions in cell death, and spontaneous activity. However, at the same time, these brains did not display organized large-scale activity, or in other words, though neurons remained alive and somewhat functional, these brains did not do anything resembling thought, sensation, perception, or anything of that nature, thankfully sidestepping most potential ethical issues.
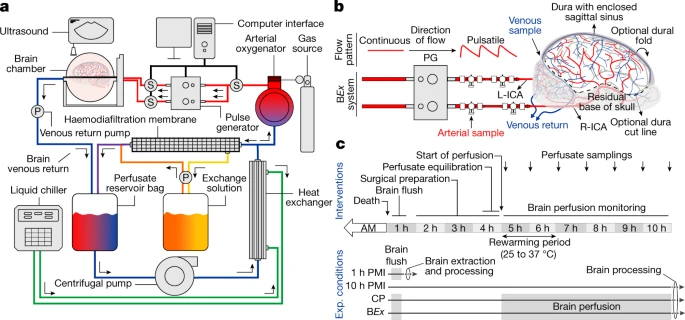
How pig brains in a vat are preserved. As you can see, it’s pretty simple and straightforward. Source: Nature.
So where do we go from here? The most obvious path forward would be to improve the above preservation techniques. Though 6 hours of survival is an achievement, it is still quite short compared to electrophysiology, and additional progress could certainly be made. Further, these brains notably lack any ability to do anything useful once preserved: restoring large-scale network activity is also likely to be a top priority. However, if such activity is restored, then a lot of the ethical issues associated with preserved brains begin to come into play, like potential subjective experience of such brains, their rights compared to their original bodies, and when to begin or end preservation of brains and under which conditions. Answering these questions will be absolutely crucial prior to moving forward, and the impact of any future developments will be largely dependent on how they relate to the ethical considerations centering such technologies.
- Lipton, P. (1999). Ischemic Cell Death in Brain Neurons. Physiol Rev.
- Du, C., et al. (1996). Very delayed infarction after mild focal cerebral ischemia: a role for apoptosis? J Cereb Blood Flow Metab.
- Ting, J., et al. (2014). Acute brain slice methods for adult and aging animals: application of targeted patch clamp analysis and optogenetics. Methods Mol Biol.
- Lee, B.R., et al. (2020). Scaled, high fidelity electrophysiological, morphological, and transcriptomic cell characterization. bioRxiv.
- Hacke, W., et al. (2004). Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet.
- Hacke, W, et al. (2008). Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke. New Engl J Med.
- Albers, G.W., et al. (2018). Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. New Engl J Med.
- Gilbert, M., et al. (2000). Resuscitation from accidental hypothermia of 13·7°C with circulatory arrest. Lancet.
- Hughes, A., et al. (2007). Full neurological recovery from profound (18.0°C) acute accidental hypothermia: successful resuscitation using active invasive rewarming techniques. Emerg Med J.
- Vrselja, Z., et al. (2019). Restoration of brain circulation and cellular functions hours post-mortem. Nature.

Pingback: Nyheder2020december31 - bionyt.dk