 December
09
December
09
Tags
Mal de Débarquement: The Science of Land Sickness
Recently I was lucky to spend seven days on a catamaran out at sea with a small group of (COVID-vaccinated) friends. We traveled around the Gulf of California, witnessing truly amazing sights like manta rays jumping out of the water, sea birds diving into the water, and turtles floating along in the swell. This was a truly novel and spectacular experience for me, although admittedly there were times when I was quite miserable. Throughout my life, I have been extremely prone to motion sickness (read a previous NeuWriteSD post on motion sickness here). So much so that even playing video games often makes me queasy. So not too long after starting the trip, unsurprisingly, I began to feel terrible. Just when I had begun to regret coming on the trip, however, my brain seemed to adjust to the constant swaying and rocking of the boat, and I no longer felt nauseated. I had gained my sea legs – it was a miracle!

Still, at the end of the week I was relieved to return to steady ground. But little did I know, my motion sickness troubles weren’t over. In the middle of the night of our return, when I woke up to get out of bed, I nearly fell over. It was dark, and in the haze of my sleepy mind I thought that we had gotten back on the boat for some reason. Everything was swaying and bobbing just as it had been out on the water – apparently, I still had my sea legs. As my thinking became more clear, I realized that my brain had gotten so used to the constant motion on the boat that it now seemed to expect it and even produced the sensations of rocking and bobbing I felt on the water. I was experiencing land sickness.
Thankfully, this unenjoyable experience faded after a few days, but I was curious: what was happening in my brain to first adapt to the constant motion, and then to feel that motion even when it wasn’t present? Why did this intense sensation of movement begin not immediately after I got off the boat, but rather after a night’s sleep on solid land?
Mal de Débarquement
This experience is often referred to as Mal de débarquement (MDD), which is a French term that means “sickness of disembarkment” (“mal” is actually the Latin root word meaning evil – an apt description, in my opinion!). While people have surely known about this for as long as we’ve been getting on boats and ships, the first known written reference was made in 1796 by Erasmus Darwin (the grandfather of naturalist Charles Darwin):
“Those, who have been upon the water in a boat or ship so long, that they have acquired the necessary habits of motion upon that unstable element, at their return on land frequently think in their reveries, or between sleeping and waking, that they observe the room, they sit in, or some of its furniture, to librate like the motion of the vessel. This I have experienced myself, and have been told, that after long voyages, it is some time before these ideas entirely vanish. The same is observable in a less degree after having travelled some days in a stage coach, and particularly when we lie down in bed, and compose ourselves to sleep; in this case it is observable, that the rattling noise of the coach, as well as the undulatory motion, haunts us.”
https://www.mdds.org.uk/history/
MDD is actually normal for a few days after an experience like mine on the boat. Sometimes, albeit much more rarely, it persists for months or longer, at which point it can be quite debilitating and is called a syndrome. Even more strangely, this syndrome can also occur spontaneously, without any motion triggers at all. While we still don’t know exactly why or how these variations of MDD occur, researchers have developed some theories. For the sake of simplicity, this article will focus on the two major theories for what is happening in the brain to cause the symptoms of motion-triggered MDD.
Theories
Maladaptation of vestibulo-ocular reflex
The first major theory involves the vestibular system, which is how our brains maintain a sense of balance and spatial orientation so we can coordinate our movements through space. It is thought that people suffering from MDD have undergone a maladaptation to their vestibulo-ocular reflex, which is a critical reflex we rely on constantly to stabilize our gaze as we move throughout the world. This reflex generates compensatory eye movements in response to head movements. In other words, when our head moves, our gaze is kept still, allowing us to keep a steady perception of the space around us. Without it, we wouldn’t be able to read signs or recognize faces while moving around. You can test this reflex by shaking your head while reading these words; if you can still read comfortably, that is the vestibulo-ocular reflex at play! On the other hand, if you were to shake the page or screen in a similar fashion, it should be much harder to read. Our vestibular system uses information about head movement along with visual signals to stabilize our gaze – with only visual signals and no motion signals, our visual processing is much less effective.

To understand what’s going wrong with the vestibulo-ocular reflex in MDD, we need to know a little about how the brain perceives head motion. This happens in the inner ear, in the vestibular labyrinth. This fancy-sounding organ contains structures for detecting rotational head movement called the semicircular canals (each of which detects rotation in a different plane), and for translational or linear head movement called the otolith organs (including the utricle and saccule). These structures are filled with a fluid called endolymph. When the head moves, taking the labyrinth along with it, the endolymph momentarily lags behind, exerting a force on sensory receptors called hair cells. This force sends a signal to the brain and is perceived as head movement.
To have a more intuitive understanding of this idea, imagine a cup of coffee on a tabletop. If you can focus on a particular bubble on the surface, or a pattern drawn on the milk foam, even better. If you slowly twist the cup around, you’ll notice that the coffee will tend to keep its initial orientation in space (it rotates in the opposite direction). Eventually, however, the coffee will catch up and rotate with the cup. It is this initial counter-rotation of the liquid in the vestibular labyrinth that exerts a pressure on the hair cells, alerting the brain to a rotational head movement [1].
Importantly, for an intact vestibulo-ocular reflex the brain needs to be able to distinguish between different types and combinations of head movements, including rotations and translations, to know when either or both are happening. Doing this successfully requires precise and complex calculations from cells in the brain’s cerebellum. When there is a mismatch between visual signals and motion signals, such as in complex motion environments like on a boat, the brain has a harder time accurately distinguishing these movements. It can take a few days of experiencing this constant complex motion for the vestibular system to get adapted. However, when that complex motion is no longer present, the system is then out of alignment for what the brain perceives as vertical or horizontal motion, resulting in sensation of motion that isn’t actually happening. Usually, the system re-adapts itself after a few days, but in rare cases it does not.
The first effective therapy for people with persistent MDD syndrome was published in 2014 by Mingjia Dai, and aims to readapt the vestibulo-ocular reflex. Briefly, subjects were treated by rolling the head from side-to-side while watching a rotating full-field visual stimulus. Promisingly, 70% of them had substantially improved symptoms for one year, though after that first year many people’s symptoms returned [2,3].
Entrainment of the entorhinal cortex
The second major theory for what causes MDD involves a concept called entrainment, which in neuroscience (and biology as a whole) is the idea that something that varies rhythmically, such as the signaling of brain cells, gradually falls into synchrony with the rhythm of something else. In this theory, a region of the brain called the entorhinal cortex becomes entrained by the rhythmic motion of the MDD trigger (such as the bobbing and swaying of the boat), which in turn alters the dynamics of signaling throughout the brain.
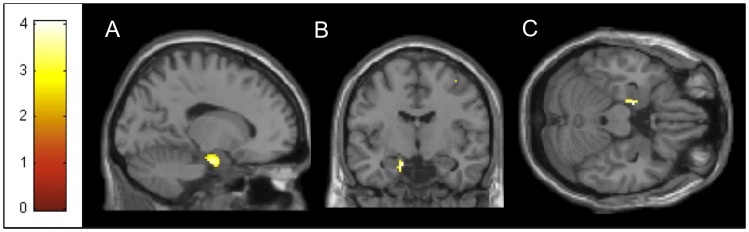
The entorhinal cortex is a central hub of spatial information processing located in the temporal lobe, and connects extensively to other brain areas, giving it a heavy influence on large-scale brain networks. So when the entorhinal cortex signaling rhythm gets synchronized with the motion trigger, this alters the communication between the entorhinal cortex with other brain areas, particularly sensory processing areas, and is thought to result in general over-synchronization of brain activity. In fact, some studies have shown efficacy of using repetitive transcranial magnetic stimulation (rTMS) to disrupt this over-synchronization in patients with MDD syndrome and improve their symptoms, although these improvements are short-lived [5,6].
Interestingly, this theory could also explain why many people with MDD don’t start having symptoms until after a night’s sleep (which was the case in my experience). The entorhinal cortex plays an important role in consolidating memories during sleep, as its cells help keep the hippocampus (a brain region important for learning and memory) active during sleep when the rest of the cortex has shut down [7].
Still a mystery…
These two theories are not mutually exclusive – it’s possible that both are true to some extent and are connected in some way. Importantly, while vestibular re-adaptation therapy and rTMS have shown some promise in helping alleviate symptoms in some people with persistent MDD, these improvements are often temporary, and there are many people who don’t respond at all to these treatments. Clearly, our understanding of exactly how MDD occurs is still limited.
There are a few other treatments that have been quite effective for some patients, which may serve as additional clues in helping researchers figure out what’s causing MDD and how to cure it. First, there is evidence showing a connection in people suffering from MDD syndrome with vestibular migraines [8], especially in cases of spontaneous MDD (where there was no motion trigger) [9]. Indeed, some of these patients have responded well to being treated with migraine lifestyle changes and medication [10]. Further, antidepressants and benzodiazepines have been highly effective in alleviating MDD symptoms [11]. Benzodiazepines are commonly used to treat anxiety disorders, and work primarily by increasing the effects of GABA (a natural inhibitory chemical in the brain), causing a sedative effect. Many cases of spontaneous MDD actually happen to occur during periods of high stress or anxiety, which can trigger hormonal changes in the body that might play a role in the onset of MDD. Antidepressants, including SSRIs and SNRIs, increase the effects of another important brain chemical, serotonin. Serotonin has been shown to reduce signaling in some hippocampal neurons [12], which as I mentioned earlier are hyperactive in MDD.
Personally, despite my unfortunate luck with getting both sea and land sickness, I am extremely thankful that these experiences were temporary, and I would 100% take this trip again.

References
[1] Kandel ER, Schwartz JH, Jessell TM, Siegelbaum SA, Hudspeth AJ. Principles of Neural Science. Fifth edition. New York, N.Y.: McGraw-Hill Education LLC., 2013.
[2] Dai M, Cohen B, Smouha E, Cho C. Readaptation of the vestibulo-ocular reflex relieves the mal de débarquement syndrome. Front Neurol. 2014;5:124. Published 2014 Jul 15. doi:10.3389/fneur.2014.00124
[3] Dai M, Cohen B, Cho C, Shin S, Yakushin SB. Treatment of the Mal de Debarquement Syndrome: A 1-Year Follow-up. Front Neurol. 2017;8:175. Published 2017 May 5. doi:10.3389/fneur.2017.00175
[4] Cha YH, Chakrapani S, Craig A, Baloh RW. Metabolic and functional connectivity changes in mal de debarquement syndrome. PLoS One. 2012;7(11):e49560. doi:10.1371/journal.pone.0049560
[5] Shou G, Yuan H, Urbano D, Cha YH, Ding L. Changes of symptom and EEG in mal de débarquement syndrome patients after repetitive transcranial magnetic stimulation over bilateral prefrontal cortex: a pilot study. Annu Int Conf IEEE Eng Med Biol Soc. 2014;2014:4294-4297. doi:10.1109/EMBC.2014.6944574
[6] Yuan H, Shou G, Gleghorn D, Ding L, Cha YH. Resting State Functional Connectivity Signature of Treatment Effects of Repetitive Transcranial Magnetic Stimulation in Mal de débarquement Syndrome. Brain Connect. 2017;7(9):617-626. doi:10.1089/brain.2017.0514
[7] Dupret D, Csicsvari J. The medial entorhinal cortex keeps Up. Nat Neurosci. 2012;15(11):1471-1472. doi:10.1038/nn.3245
[8] Cha YH, Cui Y. Rocking dizziness and headache: a two-way street. Cephalalgia. 2013;33(14):1160-1169. doi:10.1177/0333102413487999
[9] Cha YH, Brodsky J, Ishiyama G, Sabatti C, Baloh RW. Clinical features and associated syndromes of mal de débarquement. J Neurol. 2008;255(7):1038-1044. doi:10.1007/s00415-008-0837-3
[10] Ghavami Y, Haidar YM, Ziai KN, et al. Management of mal de débarquement syndrome as vestibular migraines. Laryngoscope. 2017;127(7):1670-1675. doi:10.1002/lary.26299
[11] Cha YH, Cui YY, Baloh RW. Comprehensive Clinical Profile of Mal De débarquement Syndrome. Front Neurol. 2018;9:261. Published 2018 May 7. doi:10.3389/fneur.2018.00261
[12] Dale E, Pehrson AL, Jeyarajah T, et al. Effects of serotonin in the hippocampus: how SSRIs and multimodal antidepressants might regulate pyramidal cell function. CNS Spectr. 2016;21(2):143-161. doi:10.1017/S1092852915000425

You must be logged in to post a comment.